“To hell with sitting in this meeting. Shut up! Stop talking!” Sibongile Tshabalala, fresh with grief over the recent death of irreplaceable activist Prudence Mabele launched the International AIDS Society meeting in Paris this week with a burning call to action and tribute to both Prudence and activist physician Mark Wainberg. Both, she said, would want far less talk and far more action. She led participants in the Prudence Pledge—which included the essential commitment to be “innovative, unconventional and inconvenient in our approaches to ending the AIDS epidemic.”
Meeting participants stood to take the pledge—and yet the meeting itself continued, one in a field that is now entering its third decade of annual IAS meetings: we feel there’s too much talk, yet we sometimes need to gather in shared grief and to rekindle the fire needed to keep fighting.
And perhaps that’s the task of this, and every, AIDS conference: to hold multiple realities at the same time. There is good news and bad news, often in the same story. There is promise in what’s available today—this is the first meeting where people are reporting on daily oral PrEP delivery, rather than the potential of this new tool. But daily oral PrEP isn’t a magic bullet; and there’s a need to continue finding new tools, too.
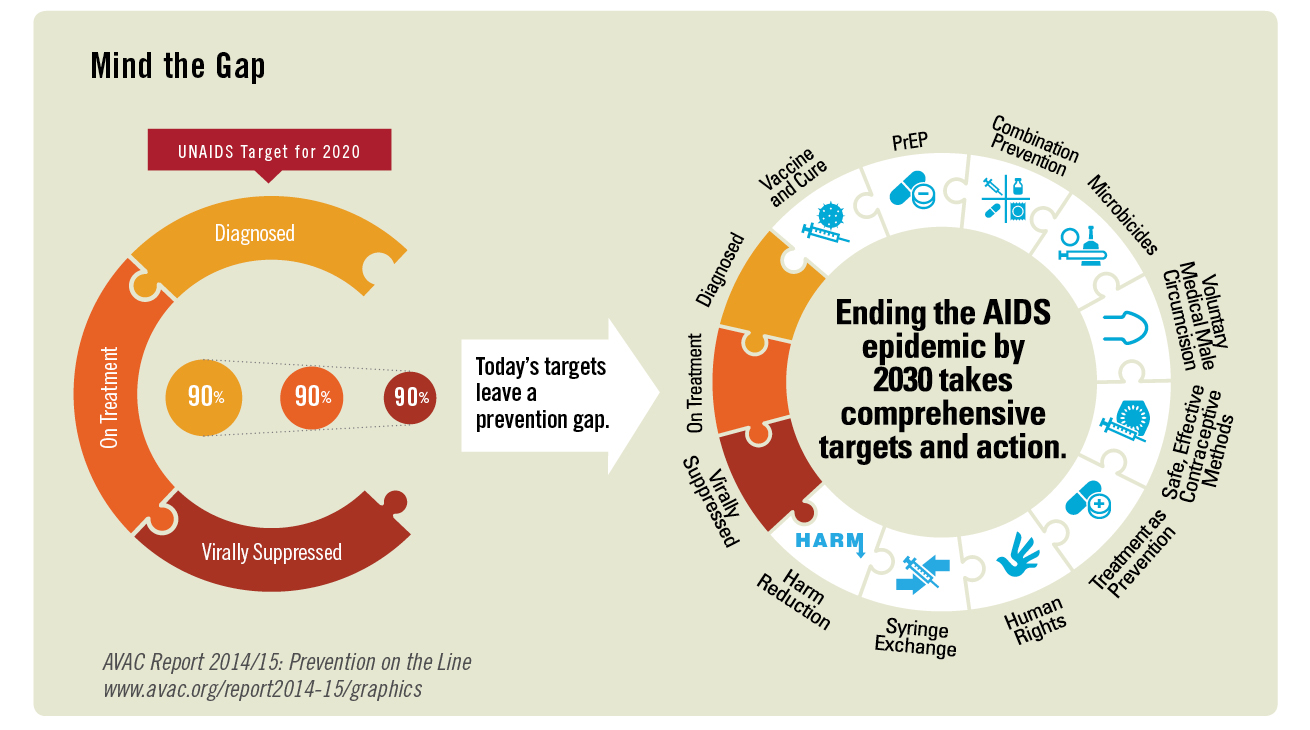
An early good news story—first promoted by UNAIDS in its annual progress report last week—that the world is making progress in achieving the 90-90-90 goals, and that these targets (90 percent of people living with HIV knowing their status; 90 percent of those people on ART; and 90 percent of those on ART virologically suppressed) will carry the world towards ending epidemic levels of HIV.
This good news was amplified on Monday with a presentation from the Swaziland Ministry of Health on the 2016 Swaziland HIV Incidence Measurement Survey. Research teams went house to house and, when individuals gave consent, administered HIV tests and collected blood samples that could be tested for the presence of HIV and for viral load. This method gives a more precise, representative picture of the number of people living with HIV in a country than other approaches, such as measuring HIV among pregnant women at antenatal clinics. A survey had been conducted in Swaziland in 2011 using the same methods—providing the first opportunity to compare new HIV diagnoses and levels of virologic suppression in a community over a period where “test and treat” with antiretroviral treatment (ART) was introduced. The good news is: It worked. During a period when ART use nearly doubled, rates of new HIV diagnoses were nearly halved, and HIV virologic suppression doubled. Today, more than 80 percent of Swazi people living with HIV are on ART, and this is very good news indeed.
But is it good enough? Unfortunately, no. As we noted last week, the UNAIDS report—while generally celebratory—contains plenty of reason for concern. There are glaring gaps in primary prevention including PrEP, voluntary medical male circumcision (VMMC), comprehensive harm reduction programs for people who inject drugs, stigma reduction—an issue tackled with eloquence and urgency in the Key Populations Declaration released earlier this week. Even in treatment, the picture isn’t rosy. Overall, the world is not on track to meet Fast Track targets for treatment, either. In 2011, UNAIDS galvanized the world around a goal of universal access to ART; this year’s report shows that just over 50 percent of people living with HIV are on ART. While countries in East and Southern Africa could potentially reach their 90-90-90 targets by 2020, success depends on sufficient resources to sustain the newly achieved speed of treatment scale up. However, West and Central Africa, Caribbean, and Asia Pacific are all not on track to hit the 90-90-90 targets.
Even in Swaziland, there’s a need to look more closely. Young people were less likely to know their status, be on ART or be virologically suppressed both in 2011 and 2016. Swaziland has been rolling out a comprehensive package of interventions for the most vulnerable adolescent girls and young women under its DREAMS program—with testing as a core component. The findings would seem to suggest that there is still ground to cover in meeting the needs of girls and women—something Prudence Mabele never stopped saying.
Monday also provided a glimpse of the future of biomedical prevention trials. Hanneke Schuitemaker from Janssen presented results from the APPROACH trial of a vaccine strategy that utilizes a mosaic immunogen—synthetic viral fragments designed to teach the body to defend itself against diverse viral subtypes. This Phase IIa trial measured the safety and immune responses of various pairings of the vaccine containing the mosaic immunogen (known as Ad26, after the adenovirus vector that carries the immunogen into the body) with other “boosts”—vaccines designed to bump up immune responses. All of the trial arms were safe and immunogenic; a combination of Ad26 plus a protein boost had the highest immunogenicity. These data, plus information from the ongoing TRAVERSE trial, will inform the design of a planned efficacy trial, known as HPX2008/HVTN 705.
By the time HPX2008/HVTN 705 starts, two trials of long-acting cabotegravir (CAB-LA) should be underway. On Tuesday, HPTN 077—a study of CAB-LA in 199 men and women in Brazil, Malawi, South Africa and the US—confirmed the findings of the ÉCLAIR CAB-LA study in men: a bi-monthly set of injections with a 600-mg dose of CAB-LA leads to the blood-drug levels thought to be associated with protection; a three-monthly injection with an 800-mg dose does not. Participants continued to report injection-site reactions as discussed in our blog on long-acting injectables. However, the HPTN 077 findings confirm this strategy is safe and tolerated for men and women. In response to a press conference question on whether there were any sex differences seen in HPTN 077, investigator Raphael Landovitz noted that these studies are trying to better understand any PK differences in women and men. The injections go into a “large muscle belly”, which serves as a reservoir to essentially seed blood plasma over time. What governs the differences in drug levels observed? In ÉCLAIR, body-mass index, or BMI, seemed to be associated. In HTPN 077, researchers noted that the rate at which the drug seeps out of the muscle belly into plasma was 50 percent slower in women than in men (which also made for lower peak concentrations after the same dose). This didn’t seem to be linked to body mass index, per Landovitz. Researchers will learn more about whether this difference has any clinical significance during the Phase III large-scale studies (HPTN 083 and 084) that will look at safety and whether CAB-LA is effective for HIV prevention.
At the AVAC-organized prevention satellite on Sunday, US Global AIDS Ambassador Deborah Birx admonished the audience to work with, and on, the multiple realities of today—delivering what’s available, pursuing new options and seeing today’s daily oral PrEP investments as the foundation for a prevention platform. It’s not a contradiction—it’s a continuum.
We must see the world this way—because it’s the only way towards a conclusive end of the epidemic. As Sibongile Tshabalala said, “AIDS isn’t over!! If the party [for the end of the epidemic] starts now, the end will never come.”