Qualitative research on PrEP often hinges on interviews with study participants. The 3Ps for Prevention (Partners, Perceptions and Pills) study (3P), which evaluates PrEP use and adherence in adolescent girls and young women in Cape Town, South Africa, decided to also try an alternative methodology: incorporate photography as a way for the young women to document their experience with PrEP. Their photographs added a visual component to the research, enhanced their agency as participants in the study, and helped them to shape the conversation about PrEP. The images they created gave researchers a unique view into participants’ perspectives on PrEP, revealing new dimensions to their experience and the factors that encourage or discourage PrEP use.
PhotoVoice is a participatory research methodology that depicts personal narratives through photography. Researchers at the Women’s Global Health Imperative program (WGHI) at RTI International conducted the PhotoVoice project in partnership with the Desmond Tutu HIV Foundation (DTHF). Six young women from adherence clubs in the 3P study volunteered to participate in the project over a two-week period in July 2018. Researchers presented PhotoVoice as a tool participants could use to reflect on what motivates or deters PrEP use and adherence. At the time of the project, they had been taking PrEP for up to one year as participants in the 3P study.
By relying on visuals with brief captions as the primary mode of communication, PhotoVoice brought to light particular aspects to their experience that may not have emerged in interviews or surveys. In research studies with young people, sustaining participant interest and motivation can be difficult. This project is “a fun way to get participants more engaged,” says Shannon O’Rourke of WGHI at RTI International. “PhotoVoice taps into a different part of young women’s brain as they try to explain their experience through this PrEP journey,” says Ariane van der Straten, Senior Fellow and Director, WGHI at RTI International. “We tend to be verbal when we are conducting research – we primarily ask questions and ask participants to answer. PhotoVoice a very different process to produce images of that experience.”
The project kicked off with an initial focus group discussion and a training session by a local photographer on the PhotoVoice method and basic elements of photography. The young women participated in a series of follow up meetings where they shared their photography and discussed what they were hoping to capture about their experiences with PrEP. While the project facilitators provided some guidance, feedback and suggestions were largely offered by the participants themselves.
The project was structured around three topics – relationships, risk perception, messaging – which came through as major themes in interviews with 3P participants. Using these same themes as a guide for the photography allowed researchers to compare the images with the interviews. Participants were also encouraged to go beyond these themes and photograph anything related to their journey with PrEP, and in so doing, they drove the direction of the research. The project culminated in an exhibition at the DTHF Youth Centre in Masiphumelele, Cape Town (where the 3P study is located).
A rich array of photos were produced, highlighting how young women saw themselves in their communities and the lives they were aspiring to lead. The images explore what empowered them, what gave them a sense of belonging, and what they found challenging. In addition to taking photographs, participants wrote captions for each image, describing its significance or symbolic meaning.
Through this process, participants created their own representations of PrEP in their lives. For instance, a photo of women dancing signified how PrEP is empowering to one PhotoVoice participant. Photos depicting a partner’s distrust, worries about sexual violence, and alcohol abuse in their communities were uniquely vivid compared to verbal accounts of these situations, filtered through researchers’ written words. “I don’t think we realize the level of stress and trauma that these young women have to navigate on a daily basis – and what that translates to in terms of creating a commitment and a habit of taking pills,” explains van der Straten. “It was important to ground the words they’re saying into something that is more visually real.”

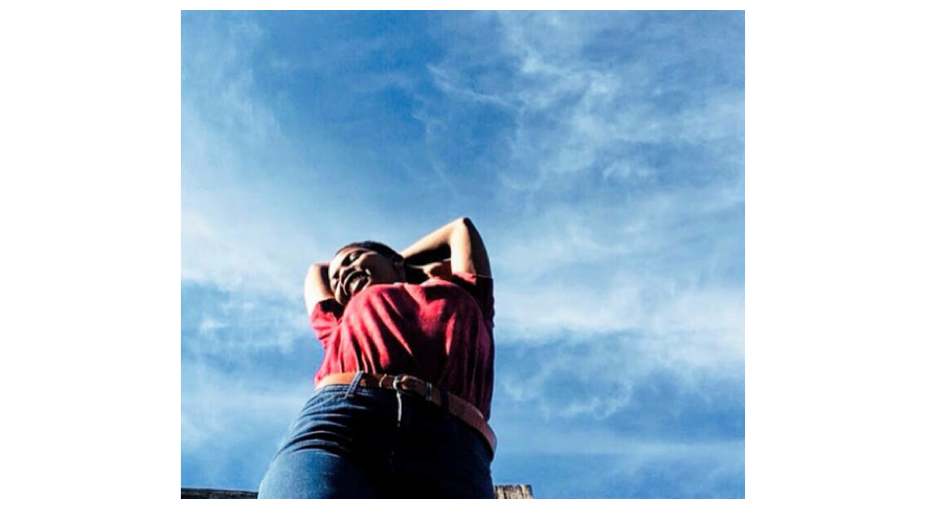
“When your partner is with you but still looks at other girls, he can put you in danger.”
These photographs enabled young women to express feelings metaphorically, expanding the range and depth of experiences they explored with researchers. A picture of plants deteriorating represents how PrEP prevents HIV in the body; another of children running along the beach shows how PrEP can help foster a fulfilling life. While talking can draw out the rationalized reasons behind the decision to take PrEP, “there is an emotional component to taking PrEP and sticking with PrEP. These pictures render better the emotional dimension that is sometimes hard to capture when we just ask questions,” says van der Straten.

“CD4 is losing power. Taking 3P (PrEP) to avoid HIV and make my CD4 strong.”
The photos and captions revealed the shifting factors that encourage or discourage PrEP use and how they change over time, depending on how long the women had been taking PrEP. Social support was fundamental for new users, with many depicting who they could count on. Family members, particularly mothers whom participants lived with, served as both strong sources of support and in some cases opposition. Those with longer term PrEP use portrayed self-motivation to take PrEP, saying it empowered them and made them feel safer in their communities. Some explored images showing the importance they attach to acting as advocates in their community.

“Support: my mom supports me all the time.”
The photos also illuminated reasons and patterns related to PrEP discontinuation. Most of the young women who stopped PrEP pointed to external circumstances that made PrEP use less feasible, rather than questioning its value. One stopped because she went through the process of becoming a traditional healer but intended to restart after her initiation in the role. Some experienced a death in the family; others had to move out of their communities. The project also highlighted the need to better understand women’s desire to stop and restart, and how to support changes in PrEP use. Those who stopped expressed that, “this is something I will look forward to do later on – just not right now,” says van der Straten.
In fact, most PhotoVoice participants reported positive experiences taking PrEP. It gave them an avenue to communicate with their partners about sexual health that they didn’t previously have. One said the PhotoVoice process allowed her to think more about why she was taking PrEP, and as a result now feels more motivated to adhere to her pills. Another felt it was important to depict her struggle with side effects in the beginning and overcoming these barriers.
“Be who you are.”
The issue of stigma was underrepresented in photos, not because it did not play a role in young women’s lives, but because it was harder for participants to take pictures of those who reject them. One, whose mother disapproved of PrEP, took a photo with her peer’s mother to illustrate a parent’s opposition to preventive pill-taking. Whereas PhotoVoice found that supportive relationships proved central to adherence and a positive experience of PrEP use; how young women internalize stigma and social opposition merits further research exploration.
The exhibition of participants’ photos at the Desmond Tutu HIV Foundation Youth Centre in Masiphumelele created a dialogue among other young women in the 3P study who came to the exhibition, as they compared their own PrEP experiences to what was depicted in the photos.
PhotoVoice proved instrumental for the 3P study and has the potential to enrich research studies more broadly. In the 3P study, PhotoVoice cued researchers early to the need to know much more about the emotional journey young PrEP users experienced. Subsequent qualitative analysis was structured to continue to explore these questions, yielding valuable insights around different types of motivations and the process of forming an identity as a PrEP user. Other studies could similarly benefit from giving participants this alternative, expressive form of self-exploration, and a participatory process to feel more engaged in co-creating the research.
Beyond research, PhotoVoice projects could be built into the design of PrEP programs to understand how PrEP users define their emotional journey and the significance of PrEP. It would allow programs to better align with what’s happening in participants’ lives and offer tailored support. And while many researchers and implementers grapple with the question of how to improve PrEP persistence rates, PhotoVoice could unearth potential solutions. “It’s a powerful tool that is not used enough,” says van der Straten. Making research more visual offers a new window into the lives of young women and, in turn, allow programs to better serve them.
For more information on the work of the Desmond Tutu HIV Foundation and RTI International’s work, see: