Join AVAC and partners as we host 24 Hours to Save AIDS Research on September 16-17. This all-day, online marathon will include more than 70 speakers from around the world sharing their work and experiences with HIV research. Registration is open and the interactive event will stream on YouTube.

Since January 20, the US Presidential Administration has been making massive cuts to HIV research, dismantling the infrastructure for conducting research and sharing misinformation on the benefits of research. The commitment and actions of the scientific and advocacy communities have been successful in reversing some of these actions and the pressure must continue.
For more ways to make the case for sustained investments in biomedical research and development and to track the devastating impacts of recent cuts on HIV and STI research and development, visit Research Matters, which shares a toolkit for researchers, and see our impact trackers below.
Impact Trackers
HIV Prevention R&D at Risk
Want to understand how the US policy shifts are endangering the future pipeline of HIV prevention tools? Check out our HIV Prevention R&D at Risk tracker.
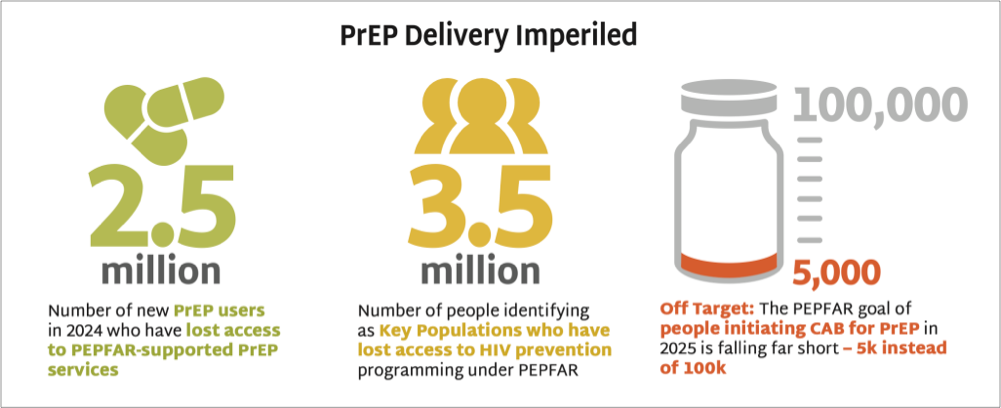
Impact of PEPFAR Stop Work Orders
Want an in-depth look at how the PEPFAR stop work orders and contract terminations have disrupted PrEP access? Check out our PEPFAR PrEP impact tracker.

Why STI Funding Matters: Worldwide Prevention, Shared Protection
Want to know about the global threat posed by defunding STI research and programming? See our Why STI Funding Matters tracker.
Delivering Lenacapavir for PrEP
As the fight to protect HIV research from devastating cuts continues, we must also push to ensure that the breakthroughs it generates, like innovative new PrEP options, reach the populations most in need of prevention.

PEPFAR Reemerges to Support Rollout of Lenacapavir for PrEP
PEPFAR and Gilead Sciences announced plans to procure injectable lenacapavir for PrEP (LEN) in “countries with the largest HIV/AIDS epidemics… with a focus on preventing mother-to-child transmission” last week. This is not new news, since PEPFAR and the Global Fund had already announced an ambition to reach two million people with LEN in the first three years—and the Global Fund recommitted to the ambition in their July announcement with Gilead. “It’s a step forward from where we’ve been in a fairly paralytic state for the last seven months, and I hope that this breaks the logjam and at least can get prevention back on the agenda,” AVAC’s Mitchell Warren told NPR.
Resources to Deliver LEN with Speed, Scale and Equity
See AVAC’s in-depth resources to inform an equitable and effective rollout of LEN.
- The Gears of Lenacapavir for PrEP Rollout: Outlines a plan to specifying priorities by stakeholder and evaluates volume and pricing strategies with near term priorities over the next few years.
- Moving a Product to the Real World graphic shows the delays in past efforts to rollout PrEP and hopeful signs for accelerated rollout this time, if we work collectively with speed, scale and equity.
- Getting PrEP Rollout Right This Time shares key insights from earlier rollouts of PrEP (such as oral PrEP) to inform a faster, smarter and more equitable introduction of LEN and future PrEP products.
- Now What with Injectable LEN for PrEP? summarizes what is actually known – and not – and what needs to happen next with LEN.
The miracle of mRNA: What’s possible beyond SARS-CoV-2—understanding mRNA, its history and potential challenges for HIV vaccines
Thursday, September 11 at 9am ET
Approved in July, lenacapavir for PrEP has tremendous potential to increase access and engagement in the United States, reaching individuals who have been unable to embrace PrEP in its previous formulations. Please join the Choice Agenda and the HIV BLUPrInt team for a deep dive into rolling out LEN in the US.