First appearing on the Lancet, Ken Mayer provides a great summary of the recent HIV R4P Conference.
At the recent HIV Research for Prevention 2014 (HIV R4P) conference in Cape Town, South Africa, almost 1400 researchers from around the world came together to discuss advances in biobehavioural HIV prevention science. The rationale for this first-time meeting was that investigators need to understand the latest research findings from a wide array of disciplines, if the most promising approaches to HIV prevention can be transformed into sustained, cohesive responses that will arrest the pandemic.
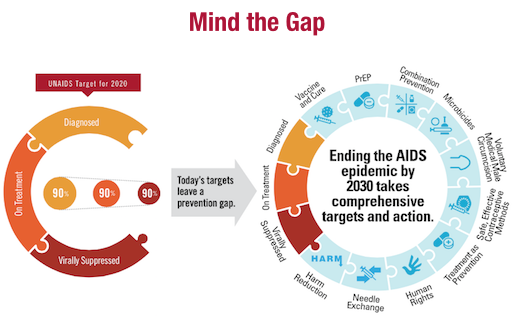
In the few years since the HPTN 052 trial showed that earlier initiation of antiretroviral therapy for HIV-infected people decreased HIV transmission to their serodiscordant partners, the concept of “treatment as prevention” has been popularised.2 Annualised global HIV incidence has decreased by a third annually since the height of the epidemic from more than 3 million to about 2 million cases per year. Four large community-randomised studies are underway in South Africa, Botswana, Zambia, Kenya, and Uganda to understand the population-level impact of earlier antiretroviral treatment combined with other evidence-based prevention services. However, initial successes have been followed by subsequent increased HIV spread in some populations. Favourable or stable national trends could mask rising HIV incidence in key populations—ie, men who have sex with men (MSM), sex workers, people who inject drugs, vulnerable youth—often due to decreased access to services because of stigma and discrimination.5 Despite annual HIV incidence decreasing over the past decade, with several million new infections a year, and with declining mortality among people living with HIV, the epidemic continues to grow. Expansion of treatment is an appropriate aspiration, but research to optimise other prevention approaches remains necessary.
During the past 5 years, seven efficacy trials of oral or topical tenofovir-based regimens used for pre-exposure prophylaxis (PrEP) to prevent HIV acquisition have been completed, with five showing efficacy. Efficacy studies in diverse populations now show that chemoprophylaxis works, but many factors can limit adherence., Investigators have learned that in trials that did not show PrEP efficacy, some participants who enrolled in PrEP trials were motivated by economic and medical incentives, did not perceive themselves at increased risk for HIV, or did not trust researchers. Just before and during HIV R4P, two newer PrEP studies, PROUD in the UK and IPERGAY in France, announced they were moving MSM participants from the control conditions (waiting list or placebo) to receive tenofovir-emtricitabine because interim analyses showed incontrovertible efficacy of tenofovir/emtricitabine as PrEP, adding new evidence that PrEP can become an important prevention tool. Further research is underway to develop culturally tailored programmes to enhance adherence for those who can most benefit from PrEP. Careful assessment of pharmacological and behavioural patterns will lead to recommendations for optimised use of PrEP, with the possibility of less than daily dosing.
Other methods of prevention discussed at HIV R4P included topical gels and intravaginal rings, which have been investigated as ways to minimise systemic antiretroviral exposures, and could be co-formulated with hormonal contraception to provide dual protection. In the next few months, the FACTS trial, a new topical tenofovir gel efficacy study, will be completed in South Africa to determine if the findings of CAPRISA 00410 can be replicated; if successful, the results should facilitate the path for licensure of the first vaginal microbicide. This advance would provide additional impetus for efficacy studies of rectal tenofovir gel to protect those who engage in anal intercourse. Two efficacy studies of intravaginal dapvirine rings, the ASPIRE and RING studies, will be completed within the next 2 years, and, if successful, will offer another method of HIV prevention. Two long-acting partenterally administered antiretrovirals, rilpivirine and cabotegravir, are in early clinical trials, and could obviate the need for daily adherence. Over the next few years, chemoprophylaxis will provide various options for HIV prevention, analogous to birth control.
A safe and effective vaccine still remains the Holy Grail for an “AIDS-free generation”, and although no breakthroughs were announced at HIV R4P, the presentations reflected increasing optimism that progress is being made. The finding in the Thai RV 144 trial that a combination of a canarypox vector boosted by HIV envelope antigens was associated with a 31% reduction in HIV transmission has led to new insights about the correlates of protection, suggesting that non-neutralising antibodies might play an important part in the prevention of HIV transmission by facilitating cell-associated cytotoxicity, enhancing phagocytosis, or by other mechanisms that need further elucidation. An efficacy trial of a Clade-C optimised combination vaccine regimen is planned to be conducted in South Africa.
The HIV R4P meeting also highlighted the role that broadly neutralising antibodies (BNAbs) might have in HIV prevention. Several antibodies have been isolated from long-term non-progressors, rare HIV-infected individuals who retain virological control after living with HIV for decades. More recently, researchers have postulated that BNAbs might be administered for immunoprophylaxis. Early studies of parenteral BNAb administration have shown safety, and efficacy studies of passive immunoprophylaxis are being planned for African infants born to HIV-infected, treatment naive mothers and for high risk HIV-uninfected populations.19 The current generation of BNAbs may not have sufficient potency, breadth, and duration to merit licensure, but proof that the administration of BNAbs could decrease HIV incidence would be a major advance for the field, since vaccine candidates could be developed using the results as benchmarks, and newer, more potent BNAbs could also be developed for immunoprophylaxis.
As highlighted at HIV R4P, resources for HIV prevention are a major concern. Until each method of prevention has well established correlates of protection, the optimal way to show efficacy is to undertake randomised, controlled trials. HIV transmission is not efficient, and since counselling trial participants attenuates the risk of HIV acquisition, thousands of volunteers are needed for each efficacy trial. This means that the costs from bench to deployment for each new product are many million dollars. HIV R4P delegates left Cape Town with renewed optimism, along with the hope that funders and the public will understand that much more research needs to be done to optimise HIV prevention.