Our team compiled a list of AVAC’s top 10 takeaways from AIDS 2026. These topics sparked discussions and ideas among our team and AVAC’s larger partner network, and will carry our work well into the future.
1. The implications of US government cuts
The implications of the US administration’s efforts to dismantle its longstanding role as the global leader in the HIV response are coming into focus – and it’s not a pretty picture.
Credit: amFAR
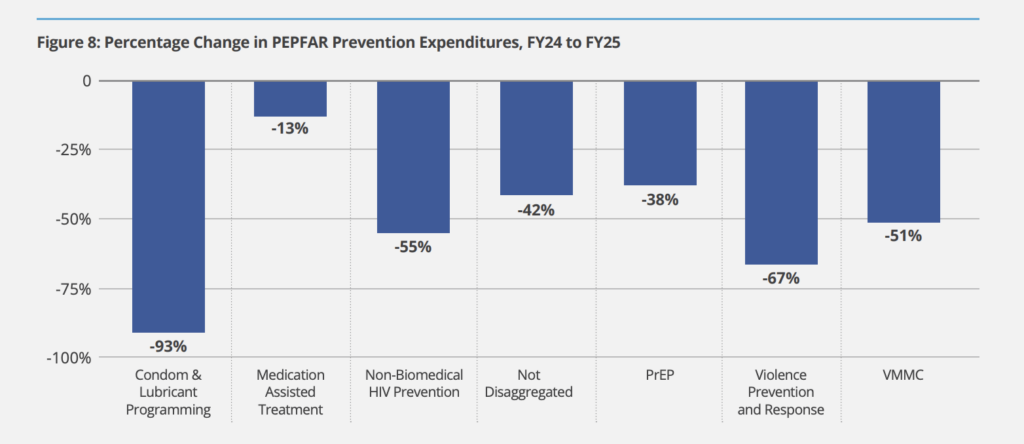
First, amfAR released a report providing the first concrete detail on the impact of PEPFAR cuts: surveying 166 organizations in 46 countries, they found that nearly 2,000 service sites had been forced to shutter.
Almost no organizations were able to fill the funding gap with other donors. Services for key populations (KPs) were “decimated”: among implementing partners, 73% stopped at least one KP service and 67% stopped outreach services.
Prevention overall took a huge hit: almost half of respondents stopped activities like condom or PrEP distribution. Two-thirds reported interruption of PMTCT and nearly one in four stopped providing prevention of mother-to-child transmission services entirely. As AVAC’s Navita Jain told POZ, when foreign aid funding was frozen, “We were in year eight of a 10-year project, really getting momentum going and accelerating prevention research, and the cuts had a massive effect, with no guidance provided or a plan for a way forward.”
As widely reported, first by former AVACer Emily Bass, and then by most major media outlets, a US State Department official displayed a mislabeled map of African countries, with African government officials in the room. As Jirair Ratevosian said, the map “should never have made it onto the screen, especially during a presentation about partnerships with African governments,” but more importantly, it’s a disappointment “that this mistake became one of the conference’s biggest media stories. Because AIDS 2026 produced important science, serious policy analysis and real progress on issues ranging from PrEP delivery to global aid transitions.”
2. Prevention innovation includes speed, scale and equity…
One of the most exciting developments arrived days before the conference, when Merck/MSD announced seven direct licenses to generic manufacturers to produce their investigational monthly pill for HIV prevention, known as alimatravir, while Phase 3 clinical trials are still enrolling.
The announcement reflects responsiveness to advocates’ longstanding calls to accelerate access to PrEP options, and deep engagement with advocates throughout the clinical trial program. Since 2012, each successive PrEP introduction has gone faster than the previous one, yet the time to market and to public health impact remains too slow.
Granting licensing agreements to generic manufacturers while clinical trials are still enrolling, before it is known if the product is effective, should significantly reduce the time to market for the product. The current timeline gives the field ample opportunity to work with ministries of health, donors, communities, and Merck to plan for broad access to the monthly PrEP pill, which lends itself to innovative delivery models – from pharmacies to community-based distribution approaches.
3. …but too often, Latin America is still left behind
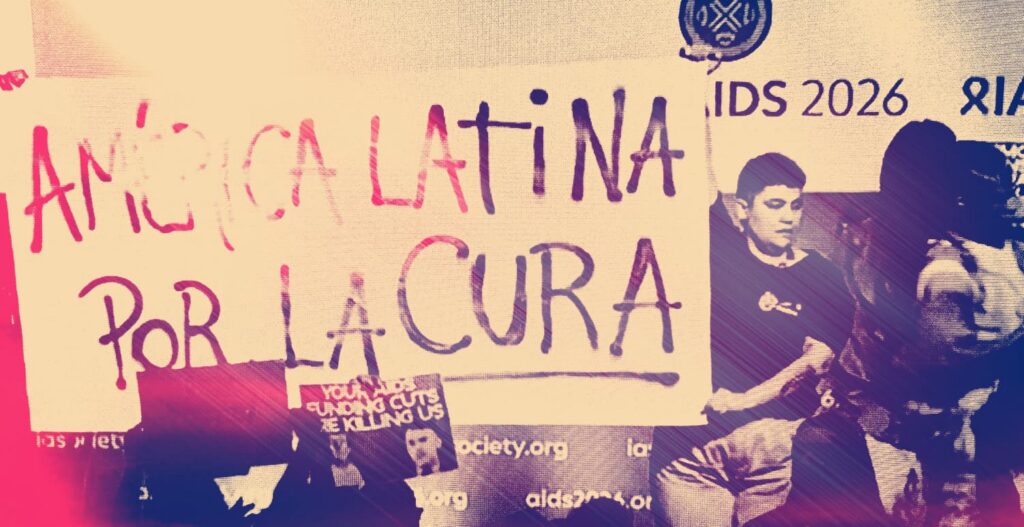
It is cruel irony that Brazil was host country to the conference, a key site for clinical trials of cabotegravir, lenacapavir and alimatravir, but has been left out of voluntary licenses for all three products.
While Merck/MSD shared information about a memorandum of understanding with Fiocruz to manufacture alimatravir for the region, the timing and next steps remain unclear: “Now is the time to plan for even speedier and wider access if alimatravir works,” said Access Bridge Executive Director Wawira Nyagah. “This must include pricing transparency from Merck and their generic licensees, accelerated investments by donors to design and implement integrated programs that offer the monthly pill as part of choice of product and service delivery models that actually reach people who need it, everywhere. This should be based on public health imperatives; not on World Bank country classifications or geographical location. Anywhere the HIV epidemic is increasing must be included, full stop.”
4. Innovative delivery and community involvement are expanding access…

AIDS 2026 showcased exciting models for HIV prevention service delivery that are removing barriers to access, reducing stigma and burden on healthcare systems. In São Paulo, vending machines delivering HIV tests, PrEP and PEP are available in subways, normalizing widespread access to HIV prevention.
Sri Lanka and the Ukraine have introduced mobile PrEP delivery programs, and in Kenya and South Africa, pharmacy delivery is reducing the load on health clinics following the drastic cuts to PEPFAR service delivery programs. The recently launched SCALE-IT project in Zambia is implementing a model for community-based delivery of PrEP options, including injectable PrEP, with more information expected soon. As we look ahead to alimatravir, the potential for a monthly PrEP pill opens the door to innovative delivery models. While alimatravir trials are still enrolling, AVAC has called on the stakeholders to ensure models are well-conceived and planned, adequately funded, and set up for success. With this timeline in hand, there’s no excuse for getting it wrong.
5. …but supply issues pose a serious threat to LEN rollout.
From countries across the globe, the same message echoed across AIDS 2026: there is demand for LEN now and the current supply is not enough. While recent commitments from PEPFAR and the Global Fund are encouraging, demand is rapidly outpacing supply across the globe – and there is an urgent need from donors to address bottlenecks and place more orders.
Access Bridge’s Nyagah reinforced this point: “People are being offered products that fit their lives, but the systems are not growing fast enough to supply it.” If supply issues are not urgently addressed, the field risks losing the demand, community trust, and current progress in LEN uptake that we have collectively worked so hard to achieve. For more on this topic, Jon Cohen’s recent piece in Science provides a deep dive into the challenges facing LEN rollout in South Africa and Zambia amidst the current political and funding landscape.
6. The urgency of vaccines: advancing the science, deepening our understanding
At a plenary session, Sandhya Vasan described why a vaccine is still needed, even with expanded PrEP options like lenacapavir, echoing AVAC’s recent commentary on the scientific challenges and emerging insights in the vaccine field and what’s in the research pipeline. Vasan highlighted long-standing partnerships with communities as foundational to vaccine research and vaccine confidence, as well as the need for continued investment and support for upstream vaccine research.
Community engagement was on full display at the HIV Cure & Prevention Research Networking Zone, where one of the best-attended sessions was the People’s Research Agenda Think Tank on HIV vaccines. AVAC’s resources on preventive vaccines and bNabs explain the science behind vaccine research.
In addition, the CAPRISA team announced results from the CAPRISA 012c Phase 2 trial examining a potential combination of two broadly neutralizing antibodies (bNAbs) as prevention. The trial found that a six-monthly combination of the CAP256 and VRC07 bNAbs was safe but did not provide protection against HIV acquisition in young women in South Africa and Zambia. As AVAC Executive Director Mitchell Warren noted, “We had hoped that combining two bNAbs in this study would provide greater protection than a single antibody, but sadly it did not.” Antibody research has always been about more than product development – research shared at the conference continues to deepen the understanding of HIV and the immune system and will continue to inform the next generation of vaccine and cure strategies.
7. Cure took another step forward
Two case presentations at the conference shared two more patients with HIV and cancer were cured following stem cell transplants for cancer treatment.
As AVAC’s senior program manager for HIV cure, Jessica Salzwedel says, “Thirteen people have now been cured via stem cell transplant. Every cure is an exciting step forward, but we must stay focused on the inequity of all 13 of these occurring in high-income countries – and ensure that our work expands access to cure information, research opportunities, and solutions.”
Cure strategies must go well beyond the science: efforts must include confronting the stigma of HIV and expanding research advocacy and engagement, especially in Africa. At pre-conference and conference sessions, along with a session at the HIV Cure & Prevention Research Networking Zone, attendees explored promising elements of the “kick and kill” strategy, gene editing technologies, the role of broadly neutralizing antibodies in “control” strategies, and how community members can get more involved.
8. Harnessing the power of AI for HIV while centering communities in the response

Many sessions explored the promise of AI to strengthen design and delivery of HIV programs, while highlighting potential pitfalls if we neglect to prioritize transparent regulatory frameworks and partnership with communities in the design, use, and oversight of AI systems.
ITPC Executive Director and AVAC Board member Solange Baptiste noted the urgency of approaches to AI that are human-centered: “We need a community governance layer built into the AI ecosystem…one that ensures communities help shape priorities, oversee the implementation, identify harms and hold systems accountable throughout the AI lifecycle.” The final plenary of the conference for the first time included a presentation on AI by Global Fund’s Izukanji Sikazwe, highlighting the dangers when the right innovations fail to scale and balancing the concept of AI as a partner with the risks AI can bring. For more insights from AVAC on the evolving discussions around AI, check out our quarterly AI and HIV Newsletter and Advocates Guide to AI and HIV Programs.
9. Partnerships power the HIV response by advancing community-centered priorities

As the field faces devastating funding cuts, strong partnerships between national, regional and global advocates are more important than ever. AVAC’s partnerships underpinned so much of the critical work discussed at AIDS 2026: to ensure key populations are not left behind, to advance community-led monitoring and community-based delivery, and translate choice into impact.
In each case, success was made possible by bringing together diverse stakeholders with the singular goal of developing innovative, community-centered approaches to the HIV response. As AVAC’s Warren reflected following the conference, “Communities are the leaders of AIDS programming. All over the conference they led plenaries, symposia, abstracts. These are not recipients, they are leaders who are driving the conversations.”
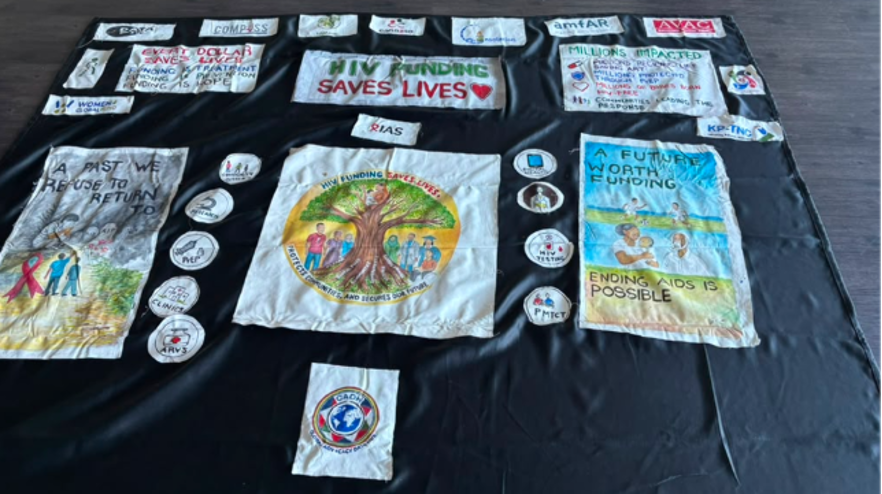
10. Communities are the heart of the AIDS response, and the Global Village is the heart of the AIDS conference.

In conversations, meet-ups, and protests coordinated across the Global Village, the power of advocates and coalition-based advocacy was a key theme of the conference. AVAC’s HIV Cure and Prevention Research Networking Zone brought delegates, researchers, advocates, and community members together for interactive discussions, expert-led sessions and networking conversations.
The Zone featured the “HIV Funding Saves Lives” quilt created by COMPASS and the Global Advocacy Data Hub to convey the impact of funding cuts on communities. Attendees signed the quilt, adding their voices to the demands for HIV funding to be restored. As advocates look ahead, connections built at the Networking Zone will strengthen for future coalition-based advocacy.