What We Protected. What We Accelerated. What Comes Next.
“In this moment of crisis and possibility, AVAC did what it has done for 30 years: We showed up, spoke out and worked with partners to push the field forward.”
— Mitchell Warren, Executive Director
In a year marked by funding freezes, political disruption and historic scientific breakthroughs, we are proud to share our 2025 Year in Review — one defined by crisis and resilience.
The last year tested global health in unprecedented ways. AVAC showed up: helping protect hundreds of millions of dollars for global health; defending HIV programs and research; delivering trusted data, tools and analysis; and accelerating equitable access to innovations, like long-acting PrEP.
None of this would have been possible without you — our partners, our donors, and our community.
How AVAC equipped advocates, researchers, and partners with the context and tools needed to understand and act in a volatile environment.
How our legal action and advocacy helped unlock global health funding – and hold the US Administration accountable.
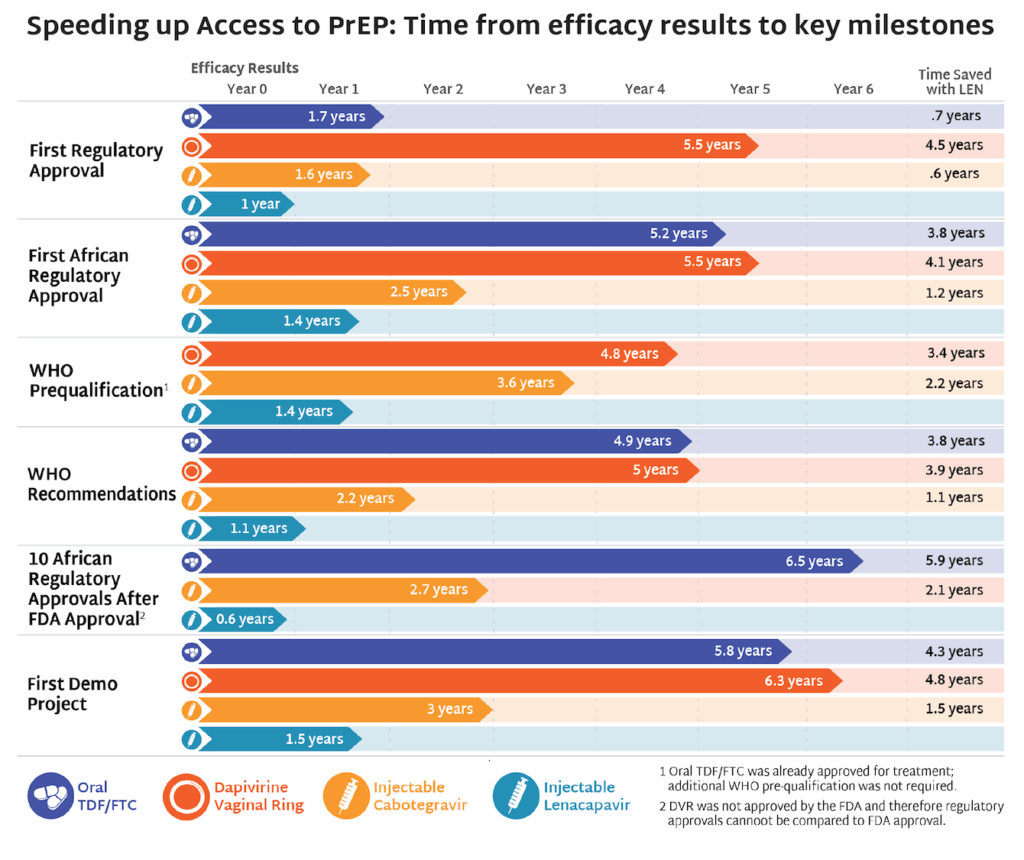
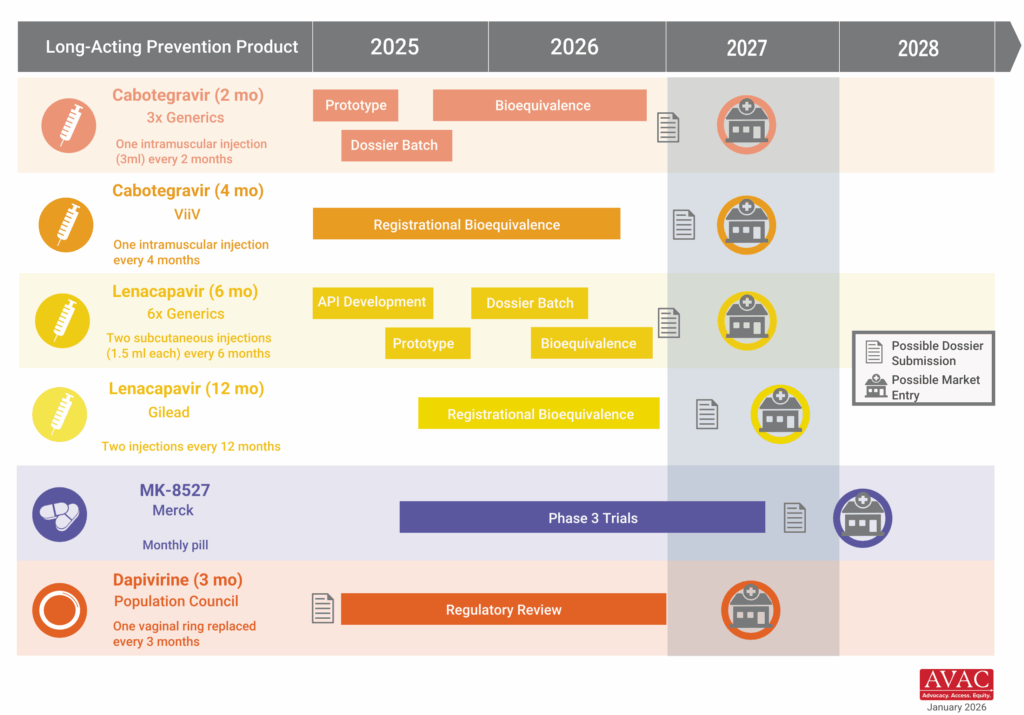
What it took to move lenacapavir for PrEP (LEN) faster into the market than any prevention product before it.
Why defending global health requires sustained vigilance, strong leadership and robust partnerships.
AVAC — like the field at large — enters 2026 in transition. We stand ready for the future: supporting African leadership, strengthening bridges from R&D to delivery, and preparing for a new chapter as we move forward into our fourth decade as an organization.
As we look ahead, challenges remain. But the science is strong, new options are in the pipeline, and, with smart analysis, rigorous science, good policies and global partnerships, progress is possible — and essential. Thank you for standing with AVAC and helping to shape what’s next for HIV prevention, R&D and global health.
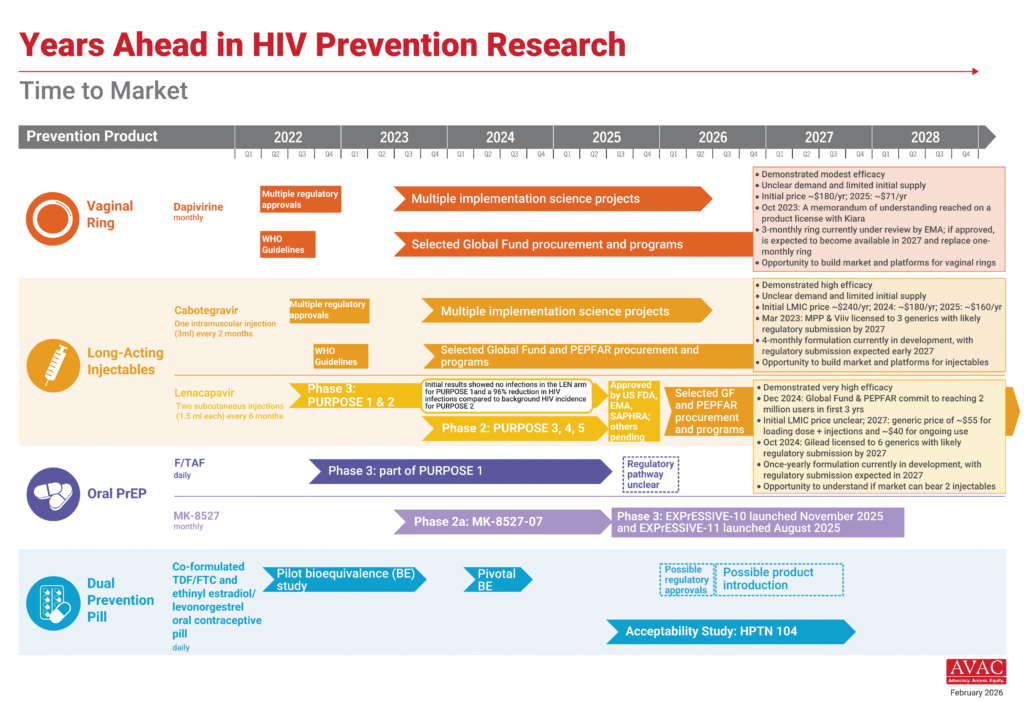
For those presenting at CROI (as well as anyone interested in tracking the field), AVAC’s latest infographics on HIV R&D and the delivery pipeline, the current landscape of prevention options, and the impact of US funding cuts are available here in an easy-to-use slide format. We hope these visuals are useful for presentations and discussions at the conference and beyond.
Each day during CROI, AVAC, EATG, Fiocruz, TAG, and other partners will host virtual webinars called Community Breakfast Clubs featuring researchers and advocates breaking down important prevention, treatment and cure science presented at CROI and the implications for the field. Registration is open to all.
AVAC will be tracking news and developments from the conference. Be part of the conversation by following AVAC on BlueSky at @hivpxresearch.bsky.social, and sign up for our Advocates Network newsletters if you were forwarded this email. And be sure to follow our partner, Aidsmap, as they report from the conference.
Sessions of Interest: What to watch
Check out the CROI program for sessions of interest. Some of the things we’re watching include:
Sunday, February 22
Scott Hammer Workshop for New Researchers
Clinical Trial Design and Analysis Workshop
Opening Session with Named Lectures by Sharon Lewin, Peter Staley and Linda-Gail Bekker
Monday, February 23
Plenaries on Meeting the Moment: HIV Treatment and Prevention and Structure, Function, and Inhibition of the HIV Capsid
Sleepless in Denver: Impact of Funding Changes on HIV Care
Strategic and Resilient Responses to the Funding Crisis Across Africa
Tuesday, February 24
Plenary on Cutting-Edge Issues in Sexually Transmitted Infections
HIV Reservoirs and Cure Strategies
Counting and Caring for Transgender and Gender-Diverse Individuals
Wednesday, February 25
Manipulating the HIV Immune Response for Prevention and Treatment
From Good to Great: Advancing Treatment and Prevention
Test and Tell
Harnessing B-Cells and Antibodies for HIV Control
Some Assembly Required: Self-Blood Collection and Testing
Global Health Watch: States Sue Over Public Health Funding, Vaccine Systems Strain, Advocates Press Merck on Equitable Access
Issue 55
This week marks one year since AVAC and the Global Health Council filed their lawsuits over the sweeping foreign assistance freeze — cases that challenged the Administration’s withholding of Congressionally appropriated funds and underscored the stakes for global health and HIV programs. That broader dispute over executive power and federal spending continues to reverberate, as four US states sued the administration this week over its decision to withhold $600 million in public health grants supporting disease surveillance, emergency preparedness, vaccination, and HIV prevention. This Global Health Watch issue also examines ongoing signs of erosion in vaccine confidence and regulatory stability and calls for early global access planning for Merck’s investigational monthly oral PrEP candidate.
Four US States Sue HHS Over $600 Million in Public Health Grants
Last week, the US administration announced it would withhold approximately $600 million in previously allocated public health grants for disease surveillance, emergency preparedness, vaccination programs and HIV prevention from states it argues are not aligned with administration priorities. In response, these states, which are led by Democrats: California, Colorado, Illinois and Minnesota, filed a lawsuit against the US Department of Health and Human Services (HHS), seeking to block the cuts. The funding is primarily distributed through the US Centers for Disease Control and Prevention (CDC) and the states argue that the administration cannot retroactively impose new conditions on congressionally appropriated funds or withhold them based on policy disagreements.
IMPLICATIONS: This case mirrors broader disputes over executive authority and federal spending, including AVAC’s lawsuit, that have surfaced repeatedly over the past year. Beyond the immediate budget impact, the decision to withhold public health funds risks destabilizing prevention and preparedness systems that rely on sustained, predictable financing. For HIV and other infectious diseases, interruptions in surveillance, community outreach, and prevention programming can quickly translate into increased transmission and weakened response capacity. While $600 million in funding is on the line, so is the principle that public health infrastructure cannot function effectively if appropriated funds are subject to shifting political leverage.
Vaccine confidence continues to be undermined across multiple fronts this week. The US Food and Drug Administration (FDA) declined to review Moderna’s mRNA seasonal influenza vaccine candidate, raising questions about the regulatory pathway and timeline for review and introduction of new flu products. At the same time, the American Medical Association (AMA) announced its plans for its own independent vaccine safety and effectiveness review initiative, which signals growing concern about trusted scientific assessment processes. And a survey found declining public perceptions of the safety of COVID-19, influenza, and MMR vaccines, underscoring persistent erosion of vaccine confidence.
IMPLICATIONS: This week’s developments signal mounting stress on the scientific and governance systems that underpin vaccine confidence and access and risk fragmenting systems that were grounded in evidence and transparency. At a moment when routine immunization rates remain fragile and misinformation continues to spread, sustained regulatory clarity, transparent scientific review, and stable engagement in multilateral vaccine processes are essential to maintaining public trust and global health security.
More than 170 groups representing people living with HIV, advocates and providers across 30 countries called on Merck to commit now to a global access strategy for its investigational monthly oral PrEP candidate, MK-8527. Signatories argue that early decisions on pricing, licensing, and regulatory pathways will determine whether the product becomes a transformative addition to the HIV prevention toolkit or follows the slow, inequitable rollout patterns seen with the rollout of oral PrEP. The groups urged Merck to build on the momentum of Gilead’s accelerated work on lenacapavir and pursue regulatory pathways through the European Medicines Agency and the World Health Organization to accelerate approvals in low- and middle-income countries; seek registration in at least 10 high-burden African countries within six months of a major regulatory approval; commit to pricing at or near generic oral PrEP levels (under $40 per person per year); and negotiate non-exclusive voluntary licenses before approval to enable timely generic production.
IMPLICATIONS: This moment reinforces a lesson the HIV field has learned repeatedly: that access needs to be embedded in the design and development of new products. Decisions made during product development around pricing, licensing, regulatory strategy, and manufacturing shape whether innovation translates into impact or inequity. We are already seeing how early, proactive access planning with lenacapavir for PrEP can accelerate timelines, align donors and regulators, and drive what is now the fastest rollout of a new prevention product since oral PrEP. Advocates are pressing Merck to apply those same principles to MK-8527 now, before trials have results, to avoid the delays and disparities that have historically limited uptake of new prevention options in low- and middle-income countries.
Today marks one year since AVAC and the Journalism Development Network worked with the Public Citizen Litigation Group to sue the US President, the State Department, the US Agency for International Development (USAID), and others, seeking emergency relief from a sweeping freeze on foreign assistance issued by the incoming administration that abruptly halted life-saving global health and development programs. A parallel case was brought by Global Health Council and partners and assigned to the same District Court judge, underscoring the broad concern across the global health community.
Twelve months later, these cases have come to symbolize a much larger question: whether the executive branch can override Congress’s constitutional authority over federal spending and dismantle decades of bipartisan foreign policy with the stroke of a pen, and whether the courts and Congress will fulfill their responsibilities to serve as checks on unbridled executive power.
The past year has laid bare the real-world consequences of unchecked executive action, threatening lives, destabilizing global partnerships, and undermining the United States’ credibility as a reliable partner.
An early ruling in AVAC’s case successfully unlocked nearly $2 billion in US government payments for work already completed, affirming that the executive branch cannot refuse to spend money appropriated by Congress. But over the course of 2025, appeals by the administration, ultimately backed by the US Supreme Court, ran down the clock on $4 billion in already-appropriated funds for the 2025 fiscal year, allowing them to expire.
While the Supreme Court’s ruling did not resolve the underlying constitutional questions, the decision was narrow and the Court left open the opportunity for further argument on the merit of the questions involved. In November 2025, a joint statement to the District Court requested to pause the cases, awaiting the outcome of other relevant court decisions.
The AVAC and GHC cases remain active, but lawsuits alone cannot restore what was lost—or undo the long-term harm caused by the sudden dismantling of global health systems.
The actions by this administration demand more than concern. This moment demands public accountability, sustained Congressional oversight, and durable legislative safeguards. Global health and equity require champions willing to fight for lives and livelihoods, and for what’s right. We cannot accept this as the new normal, and we must insist that Congressional authority, democratic governance, and the lives they protect still matter.
Global Health Watch: Foreign Affairs Bill Passes, Aid Cuts Projected to Cause Millions of Deaths by 2030, UN & WHO in Financial Crisis
This week a $50 billion US foreign affairs spending bill was signed into law, averting severe proposed cuts; a new modelling analysis projects millions of additional preventable deaths by 2030 if global aid cuts continue; and the financial crises facing the UN and WHO continue. We are also following plans to transition or close the Oregon National Primate Research Center, a leading research institution that has contributed enormously in biomedical and HIV research.
US Signs Foreign Affairs Spending Bill Amid Ongoing Uncertainty
The US Congress passed the $50 billion foreign affairs spending bill and the President signed it into law Tuesday, ending a brief government shut-down. The appropriations bill restores billions in foreign assistance, along with companion bills that restore critical support for biomedical research at the NIH and domestic HIV programs, that had been at risk of deep proposed cuts, though it still represents a reduction from previous years and questions remain about how fully the administration will implement the funding and priorities laid out by lawmakers.
IMPLICATIONS: While this bill averts the most severe proposed cuts and sends a strong signal for continued engagement by Congress, the reduced funding level and uncertainty of whether global health and humanitarian programs will receive the funding Congress appropriated leave many reluctant to celebrate. Coordinated advocacy and sustained Congressional oversight will be needed to ensure all appropriated funds are obligated and spent.
A new modelling analysis published in The Lancet Global Health finds that ongoing cuts to official development assistance, particularly from long-time donors like the US, UK and Germany, could lead to between 9.4 million and 22.6 million additional deaths by 2030 across 93 low- and middle-income countries. This includes more than 5 million children under age five.
IMPLICATIONS: This analysis reinforces the need to sustain strategic investments now to avoid deaths and setbacks on all fronts, from HIV to maternal and child health to chronic diseases.
Global health and humanitarian institutions are facing an escalating financial and political crisis. UN Secretary-General António Guterres warned that the United Nations risks “imminent financial collapse” if member states, specifically the US, do not pay their dues on time, or fail to agree to revise the financial rules, which require the UN to repay governments hundreds of millions of dollars in credits for programs, even ones that were never implemented. At the same time, the World Health Organization (WHO) launched its 2026 emergency appeal amid its biggest financial decline in a decade and while the US withdrawals and other countries question their engagement.
IMPLICATIONS: While WHO and the UN pursue reforms toward more sustainable and flexible financing, failure by member states to stabilize funding and modernize governance could strip capacity from global institutions at a moment when they are needed most with major implications for health security, equity, and trust in the global response system.
NIH to Transition Primate Research Center Amid Broader Shift Away from Animal Testing
In the last week, NIH Director, Jay Bhattacharya, confirmed plans to transition the Oregon National Primate Research Center at Oregon Health & Science University (OHSU) into an animal sanctuary. This is the first of possibly seven of the NIH’s National Primate Research Centers to close or transition and is part of a broader national push to reduce animal testing. The NIH said last year it would spend $87 million to develop a standardized alternative to animal testing. OHSU’s board of directors will meet Monday to consider negotiations with the NIH. They previously estimated it would cost $241 million over eight years to close.
IMPLICATIONS: This move reflects a broader pattern of policy decisions that risk eroding the foundational research systems underpinning early-stage biomedical science, including HIV prevention, treatment, and cure research. While developing alternatives to animal research is important, rapidly dismantling animal research—particularly nonhuman primate capacity at these centers and at the CDC—without validated replacements could weaken the early-stage pipeline that has been critical to breakthroughs such as HIV PrEP, PEP, long-acting prevention, vaccine and cure research and development.
AVAC’s latest issue of PxWire shows reduced initiations of oral PrEP following the US foreign aid freeze; the accelerated rollout of injectable lenacapavir (LEN) for PrEP; and what’s next in the HIV vaccine R&D pipeline.
Impact of US Withdrawal from WHO, New Data on PrEP, Cure Academy Applications Open
AVAC Roundup
New this week: resources on the impact of harmful US policies on the HIV response; updated infographics on the ups and downs in PrEP; and an opportunity to apply for the US HIV Cure Academy in North Carolina this April.
The US withdrawal from WHO has made Americans less safe, further damaged diplomatic relationships and will ultimately make America less healthy, writes AVAC Executive Director Mitchell Warren in Positively Aware.
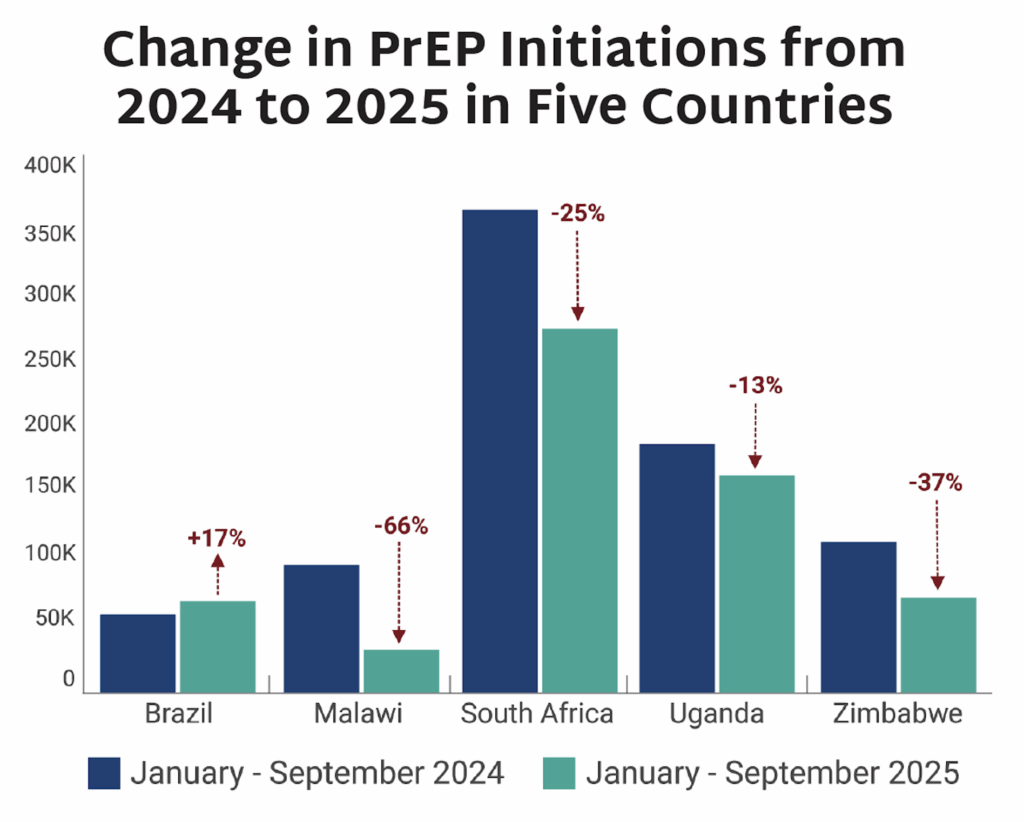
The PEPFAR stop-work order resulted in major declines in initiations of PrEP. Between January–September 2024 and January–September 2025, PrEP initiations dropped by 13-66% in high-volume countries, with the steepest declines occurring in PEPFAR-dependent programs disrupted by stop-work orders.
From Devex’s The AID Report, this article features the voices of veteran HIV advocates including AVAC’s Maureen Luba and HEPS-Uganda’s Kenneth Mwehonge. The article traces the impact of the US foreign aid freeze, illuminating how outreach, prevention and monitoring systems are fraying across four African countries critical to the HIV response.
This Bhekisisa piece explores how HIV programs must adapt after US funding cuts. AVAC’s Mitchell Warren argues that survival requires consolidation, new partnerships, boosting domestic government contributions, and sharply refocusing on HIV prevention.
The US HIV Cure Research Academy: April 22-24, 2026
The US HIV Cure Research Academy brings together researchers and community members from across the United States to learn about HIV cure science and translation. This two and a half-day intensive training program includes interactive discussions, skill-building workshops, and networking sessions. Full scholarships will be awarded for up to 15 attendees. Applications close February 13 at 11:59pm ET. Apply here: US HIV Cure Research Academy 2026! For further information please contact [email protected].
Global Health Watch: Budget stalled, Gag Rule expanded, US leaves WHO, AAP’s own immunization recommendations
Issue 53
As this issue goes to publication, the US fiscal year (FY26) budget remains unresolved in the Senate, adding to uncertainty for global health funding. A short-term funding deal reached last night would delay, but not resolve, a potential government shutdown, as negotiations over the administration’s deadly mass deportation efforts continue. For global health programs already under strain, this limbo continues to carry serious consequences. This week’s issue tracks the expansion of the Global Gag Rule under the new “Promoting Human Flourishing in Foreign Assistance” (PHFFA) policy, the US’s formal withdrawal from the World Health Organization (WHO), growing pushback on concerning vaccine policy, and the new finding that nearly half of US CDC surveillance databases have been paused or stopped.
Weaponizing Foreign Aid with the Expanded Global Gag Rule
Last Friday, the US administration expanded the harmful Global Gag Rule (GGR), also known as the Mexico City Policy, under a new Promoting Human Flourishing in Foreign Assistance policy, which broadens restrictions on US foreign aid. Originally enacted in 1984, the GGR barred non-US organizations receiving funding for global health from providing or promoting abortion services (even with their own, separate resources). Each Republican president enforced the GGR, while each Democratic president rescinded it. Now, this administration’s restrictions are being drastically expanded and extend to programs that engage in what the administration labels “gender ideology” and diversity, equity, and inclusion initiatives. It now applies not only to non-governmental organizations (NGOs) based abroad, but US NGOs, multilateral organizations and direct aid to foreign governments. Many organizations, including AVAC, Global Health Council, PAI, Planned Parenthood,Health GAP, and others called for the immediate rejection of the policy as weaponizing US foreign assistance and imposing political ideology at the expense of improving global health and international cooperation.
IMPLICATIONS: As this Think Global Health editorial from Stephanie Psaki states, “PHFFA applies not just to global health funding but to all non-military US foreign assistance, approximately $30 billion annually—or 50 times more than what was covered by the original Mexico City Policy… At best, the rules will waste US taxpayer dollars and impede the administration’s ability to implement its America First Global Health Strategy. At worst, the policy will cost lives, stall progress against key global health challenges including HIV/AIDS, and further damage US credibility with key partners—particularly across Africa.” Our colleagues at KFF, provide a very useful analysis of this latest expansion here.
As this issue was going to publication last week, the US formally notified the World Health Organization (WHO) of its decision to withdraw. This triggered responses from WHO and the United Nations noting that the US was a founding member in 1948 and a central partner in major global health gains ever since, and warning that the US departure makes the US and the world less safe.
IMPLICATIONS: The US withdrawal from the WHO underscores a deeper shift in global health governance where health is a bargaining chip for a new imperialistic ideology around foreign policy and national interest. This move heightens, rather than diminishes, the importance of multilateral cooperation. As Chatham House Fellow, Ebere Okereke, writes in Think Global Health, the “US withdrawal from the WHO increased the relevance of multilateral cooperation for Africa. The WHO remains the primary source of global health norms and coordination, even in its weakened state. Disengagement would leave African countries more exposed to power-based bargaining during crises.”
American Academy of Pediatrics Issues its Own Immunization Schedule
As US policy shifts and vaccine mis- and dis-information fuels mistrust and confusion—including this week’s chair of the CDC’s Advisory Committee on Immunization Practices (ACIP) shockingly questioning longstanding recommendations for polio vaccination—many organizations are stepping up to defend vaccine science and evidence. The American Academy of Pediatrics issued its own 2026 immunization schedule, continuing to recommend routine vaccination against 18 diseases, a broader program of vaccine protection than the new schedule of vaccines released by the US administration a few weeks ago. The AAP’s recommendations are backed by numerous professional groups including the American Medical Association and National Medical Association. The Center for Infectious Disease Research and Policy (CIDRAP) also launched an effort to boost evidence-based vaccine information by partnering with communicators and rapid-response teams to counter misinformation and clarify vaccine safety and effectiveness.
IMPLICATIONS: The AAP’s decision to publish its own comprehensive vaccine schedule, and the broad coalition endorsing it, signals a powerful pushback and commitment to evidence over ideology. This mixed guidance with the medical and scientific community differing from federal recommendations will continue to erode trust and will undermine routine immunization and confidence in public health, ultimately threatening the gains achieved against vaccine-preventable diseases such as measles, influenza, and polio.
Nearly Half of US CDC Surveillance Databases Stopped Updating
New research published in the Annals of Internal Medicine shows that nearly half of US Centers for Disease Control and Prevention (CDC) data systems have been paused. Of 82 databases meant to update monthly, 46% show unexplained pauses, most lasting six months or more, and of those paused, approximately 87% track vaccinations.
IMPLICATIONS: As Infectious Diseases Society of America (IDSA) CEO Jeanne Marrazzo writes in an accompanying editorial, “Until the United States restores the CDC and its partner agencies to their former stature, we are not only flying blind in the face of emerging and reemerging threats to human health and well-being—we are being deprived of effective weaponry.”
Roundup: Must-Read Conversations and Resources from the Last Week
Last week marked one year since the US president took office and began systematically dismantling global health and equity. Below is a roundup of essential conversations and resources summarizing the past 365 days and what’s at stake as we move forward.
READ: One Year Later: Global Health Chaos and Disruption
Last week, hundreds joined AVAC for a conversation about The People’s Research Agenda for Speed, Scale and Equity, with Jeanne Marrazzo, former NIAID Director, CEO of the Infectious Diseases Society of America (IDSA), and AVAC Board member. Watch the recording to hear what it will take to deliver science that meets the moment and how advocates can use the People’s Research Agenda, which offers a people-led framework that tracks the science, highlights where investments align with community priorities and identifies critical gaps to ensure the prevention pipeline meets the needs of diverse populations in a reimagined HIV response.
LISTEN: One year after Trump: The day HIV funding changed forever — and what came next
One year ago, Donald Trump was inaugurated as president of the United States and, overnight, US policies on HIV funding for countries like South Africa changed. Bhekisisa’s Mia Malan speaks with AVAC Executive Director Mitchell Warren to find out how international aid has changed.
READ: Fighting for Billions: The legal battle to keep US foreign aid alive
Devex’s in-depth retrospective chronicles how legal action became a critical line of defense against the dismantling of lifesaving programs by the US administration — including the ongoing cases by AVAC, the Global Health Council and partners challenging the foreign aid freeze. The piece highlights where we are with the case and why the outcome still matters.
Late on Friday, the US Administration dangerously expanded the Global Gag Rule, which further restricts the ability of organizations to engage in advocacy, education programs, discrimination protections, and legal reform, anywhere in the world, in any program, with anyone’s funding.
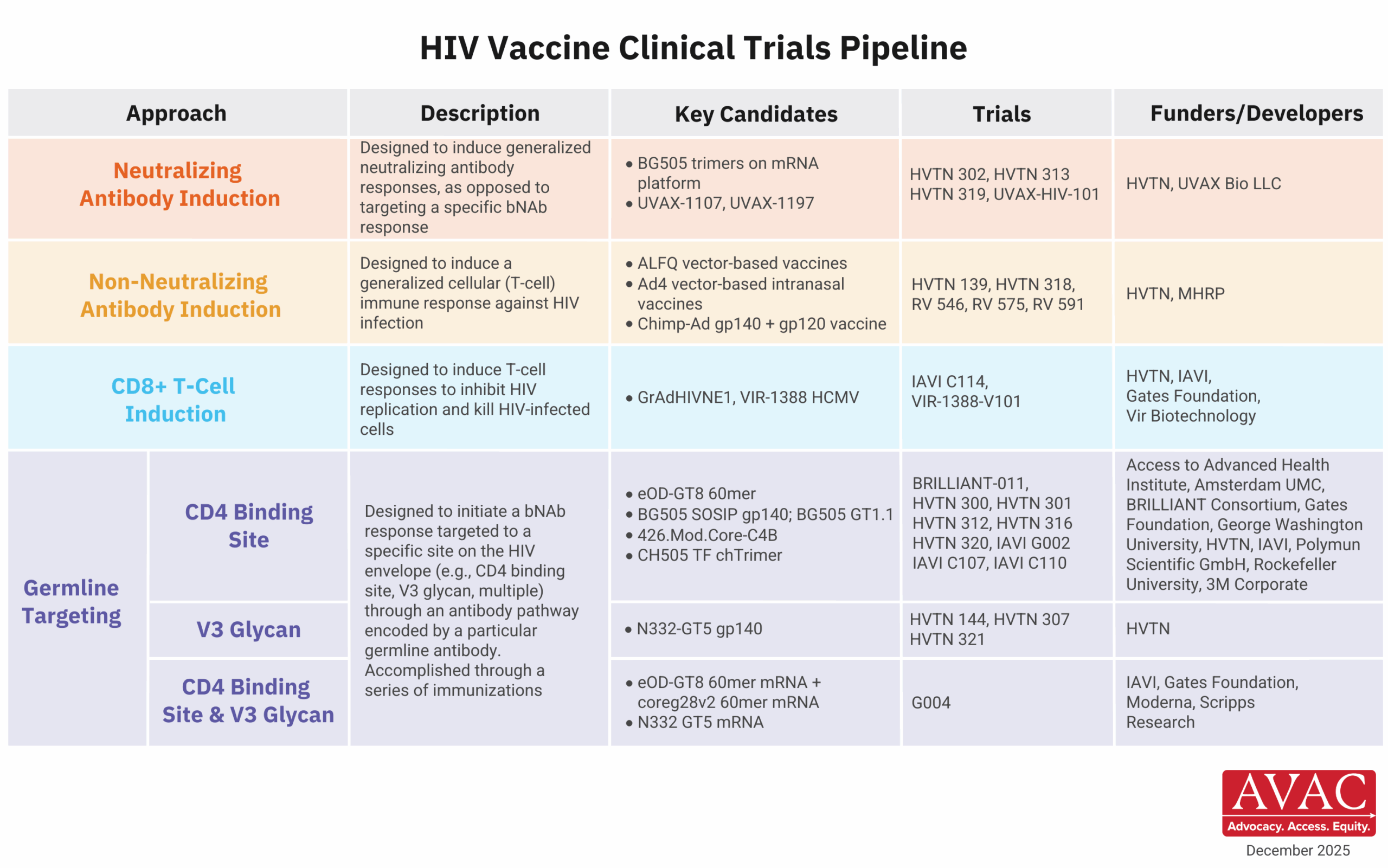
Check out three essential infographics on the HIV vaccine clinical trials pipeline, PrEP products currently available and in late-stage clinical trials and lenacapavir regulatory approvals—to visualize where the field is today and what lies ahead.
AVAC Calls for the Immediate Rejection of the Global Gag Rule and Any Expansion of it
Since first established in 1984 by President Ronald Reagan, the Global Gag Rule has harmed global health and disrupted sexual and reproductive health and HIV programs. Reports on the dangerously expanded rules likely to be issued today would move beyond the assault on women’s health and bodily autonomy and lay bare the US administration’s broader war on gender, diversity, equity and inclusion, underscoring their relentless agenda of control over people and programs.
The expanded Gag Rule restricts the ability of organizations to engage in advocacy and education programs, discrimination protections, and legal reform, anywhere in the world, in any program, with anyone’s funding. This will silence healthcare providers, undermine civil society, and deny people access to essential information and services. The expansion of this policy threatens the very integrity of evidence-based care and foreign assistance.
“This cruel Gag Rule is bad politics and bad policy,” said AVAC Executive Director Mitchell Warren. “Expanding it represents further weaponization of US funding to impose ideology at the expense of lives and livelihoods. Restricting information and activities that providers deem necessary puts individuals, communities and especially women, girls, LGBTQI+ people, and others at higher risk of poor sexual health outcomes including HIV and other infections. It also weakens the very systems required to respond to global health emergencies and prepare for future pandemics.”
People’s needs—not politics—must be at the heart of what drives US investments, programs, and global engagement. The Global Gag Rule plays politics with people’s health and lives. AVAC calls for the immediate rejection of the Global Gag Rule and any expansion of it and urges US lawmakers to uphold science, human rights, and public health.
Global Health Watch: Reflecting on 1 Year of Chaos and What’s Next, Congress Pushes Back, the Future of WHO, US Undermines African Authority
Issue 52
This week marks 365 days of disruption and chaos across global health, with many organizations and journalists reflecting on one year after the foreign aid freeze and what the future of global health looks like. This week also saw the US Congress beginning to reassert its role on health funding, ongoing US disengagement from WHO, and new reporting on the hepatitis B vaccine trial in Guinea-Bissau.
We are also watching closely for news of an expanded Global Gag Rule, that is reportedly coming out later today, just as this issue goes to press. It is anticipated that this new gag will include a dramatic expansion beyond abortion and now underscore the US administration’s war on gender, diversity, equity and inclusion. We’ll cover this in next week’s Global Health Watch; the struggle, most definitely, continues.
365 Days of Chaos and Disruption, What Comes Next for Global Health
This week marks one year since the US Presidential administration issued a deeply cruel executive order freezing foreign assistance, halting billions of dollars in already-approved funding under the bad-faith claim of a “90-day review”. What followed was not a brief pause, but a drawn-out, chaotic disruption that stopped life-saving work across the globe, shutting down valuable organizations, and harming lives, health, and livelihoods. And that was just the beginning of a year of chaos. Many organizations and media coverage noted a growing recognition that the past year’s disruptions to global health were not just destructive, but catalytic, forcing a reckoning with how systems are built and for whom. Reporting from Bhekisisa reflected on how the sudden halt in US HIV funding exposed deep vulnerabilities in over-reliance on external aid, while also accelerating conversations about domestic financing, integration, and sustainability in the HIV response moving into 2026. At the same time, analyses fromHealth Policy Watch, Science, Nature, and The Lancet laid bare the human and scientific costs of abrupt policy shifts, shuttered programs, fractured research networks, and lost trust, while underscoring that simply restoring old funding streams will not be enough to meet future challenges.
IMPLICATIONS: Together, these stories and analyses point to the need to rethink and rebuild with stronger country ownership, diversified and predictable financing, resilient research institutions, and governance structures that prioritize equity, accountability, and community leadership. Rather than recreating the same architecture, reimagined global health systems must be less dependent on external donors and political ideology. As Global Health Watch has tracked for 52 weeks, the path forward is not about returning to the pre-foreign aid freeze status quo, but about using this period of disruption to construct a more durable, equitable, and responsive global health architecture. As Canadian Prime Minister, Mark Carney, said so clearly at this week’s World Economic Forum in Davos, Switzerland, “Nostalgia is not a strategy.”
Congress Steps Up In Defending Domestic and Global Health
The US Congress is beginning to reassert its constitutional role in shaping federal spending. The joint House and Senate FY26 funding bill released last week covering foreign operations would maintain funding for core global health priorities, including HIV, tuberculosis, malaria, polio, family planning and reproductive health, neglected tropical diseases, Gavi, and UN agencies such as UNAIDS, UNICEF, and UNFPA. This week, legislators rejected nearly $2 billion in proposed cuts to US domestic HIV and related programs through the Labor, Health and Human Services Education and Related Appropriations Act (LHHS), a “major victory” credited to sustained advocacy by people living with HIV, advocates, and service providers. The proposed bill largely preserves funding for domestic public health and biomedical research. As AVAC’s Suraj Madoori said in a statement, “These crucial wins for global and domestic HIV now require us to not hold back, and urge Congress to swiftly approve all the FY26 bills, push the President to sign them, and for us to ensure accountability in the administration to spend and implement this lifesaving funding as instructed by the people and those who represent us in Washington D.C.”
IMPLICATIONS: Together, these bills signal a return to a bipartisan appropriations process and, if enacted, provide a basis to push back against unilateral cuts by the administration. They also signal bipartisan pushback against attempts to cut health and scientific research investments. By rejecting the steep cuts proposed by the administration, they stabilize lifesaving programs and protect the research enterprise. The House passed the bills on Thursday, and the focus now shifts to the Senate, which must pass the bills by January 30. Then onto the President to sign, and, most critically, for the administration to actually spend all Congressionally appropriated funds.
This week also marks one year since the US announced its intended departure from World Health Organization (WHO). Debate over its future and the US’ role within it intensified as pressure from parts of the administration collided with growing concern over the consequences of disengagement. US officials and policymakers aligned with the “America First” strategy call for WHO to be fundamentally reformed or replaced. Analysts note that the US remains a formal member of WHO until debts are paid. Meanwhile, the US administration continues to withhold funding and delay payments, leaving millions of dollars in unpaid US obligations.
IMPLICATIONS: The current state, where the US remains technically engaged but substantively absent, poses serious risks for global health governance, disease surveillance and pandemic preparedness. As analyses from CSIS underscores, WHO reform is both necessary and possible, but meaningful reform requires constructive engagement, predictable financing, and political leadership, not abandonment.
Hepatitis B Vaccine Trial in Guinea-Bissau Undermines African Authority
Reporting this week is exposing a pattern of US actions that show deep disregard for African public health leadership, ethical research standards, and sovereignty. The US-funded hepatitis B vaccine trial in Guinea-Bissau is at the center of this. As we reported in previous weeks, the unethical trial would delay birth-dose vaccination for thousands of newborns despite overwhelming evidence, and WHO guidance, that immediate vaccination saves lives. According to Rolling Stone, the study was championed by US officials aligned with anti-vaccine ideology and advanced even as Africa CDC officials raised alarm and indicated the trial should be halted. At the same time, the US administration has been marginalizing Africa CDC more broadly, cutting engagement, undermining its authority, and sidelining African institutions in favor of unilateral decision-making. This is being reinforced, as The Guardian reports, by members of the US administration urging US diplomats to emphasize American “generosity” to African leaders even as USAID programs are shuttered and health funding withdrawn.
IMPLICATIONS: Together, these developments signal a dangerous erosion of respect for African expertise, autonomy, and ethical authority in global health. Pushing forward research designs that would withhold proven interventions—while dismissing objections from Africa CDC and African scientists—revives patterns of extractive and unethical research long condemned by the global health community. Undermining Africa CDC while advancing ethically dubious trials weakens trust, damages partnerships, and threatens progress against hepatitis B, HIV, and other diseases where Africa has led with scientific excellence.
This five-part series reflects on the tumultuous events of the past 365 days across five global health issues: the erosion of US foreign aid; dismantling of the research enterprise; attacks on vaccine policy; and shifts in the global health architecture.
As new IDSA CEO, Jeanne Marrazzo warned in a webinar this week, rising HIV infections threaten progress, but “this is not a time to despair. It’s a time to fight.” Watch the recording and explore the 2025 People’s Research Agenda, which tracks the science, flags gaps, and centers community priorities to keep HIV prevention moving forward.