AVAC and 627 organizations, institutions, researchers, clinicians, public health advocates and stakeholders submitted a written letter to the Senate HELP Committee urging lawmakers to reject the cuts to NIH funding for HIV, TB, and STI research and highlighting the impact of these cuts on lifesaving innovation and research infrastructure.
Protect Federal Funding for HIV, TB, and STI Research and Prevention at the National Institutes of Health
Long-Acting PrEP Real-Time Data Dashboard
The GBGMC dashboard provides updated insights on the effectiveness of Long Acting PrEP interventions, user demographics, and access rates across regions. Visit here.
Why HIV Prevention Must Not Be Left Behind
In this presentation at the INTEREST 2025 conference, Rhoda Msiska of Copper Rose Zambia emphasizes the urgency of protecting the progress made in scaling up PrEP and the need to act now to expand access to new HIV prevention tools like injectable lenacapavir (LEN) and the Dual Prevention Pill (DPP).
Advocates’ Guide: Understanding the President’s Proposed Fiscal Year 2026 (FY26) Budget and Its Implications for Science, Research and Global Health
The US administration’s proposed Fiscal Year 2026 (FY26) budget marks a sweeping rollback of federal investment in health, research, and global development. For advocates, researchers, and implementers, this proposal demands urgent attention and action.
This initial “skinny budget” is a proposal and not yet law. A more detailed proposal will be released by mid-to-late May and the US Congress will ultimately decide actual funding levels for FY26, which begins October 1. So, advocates must speak up now to protect funding for research and programming that saves lives and livelihoods.
Here’s what advocates need to know and do:
Big Picture: A Dramatic Retrenchment
The budget proposes $163 billion in cuts to non-defense discretionary spending, including a 26% reduction to the Department of Health and Human Services (HHS)— the department that oversees the US National Institutes of Health (NIH), the Centers for Disease Control and Prevention (CDC), and the Food and Drug Administration (FDA). These cuts are completely offset by an increase to defense spending and reflect a shift toward the elimination of science and programming tied to diversity, equity, inclusion (DEI), gender, and climate, and a redirection of funding toward defense and “America First” priorities—priorities that put the perceived interests of the US and its citizens over other national and global issues.
Detailed Analysis and Implications
Health and Biomedical Research
The proposed cuts to HHS would gut federal support for health and biomedical research, dismantling key programs at NIH and CDC. They threaten progress on infectious diseases, health equity, and pandemic preparedness—undermining decades of scientific gains and leaving communities vulnerable.
NIH is Cut by $17.9 billion losing HIV and global health research
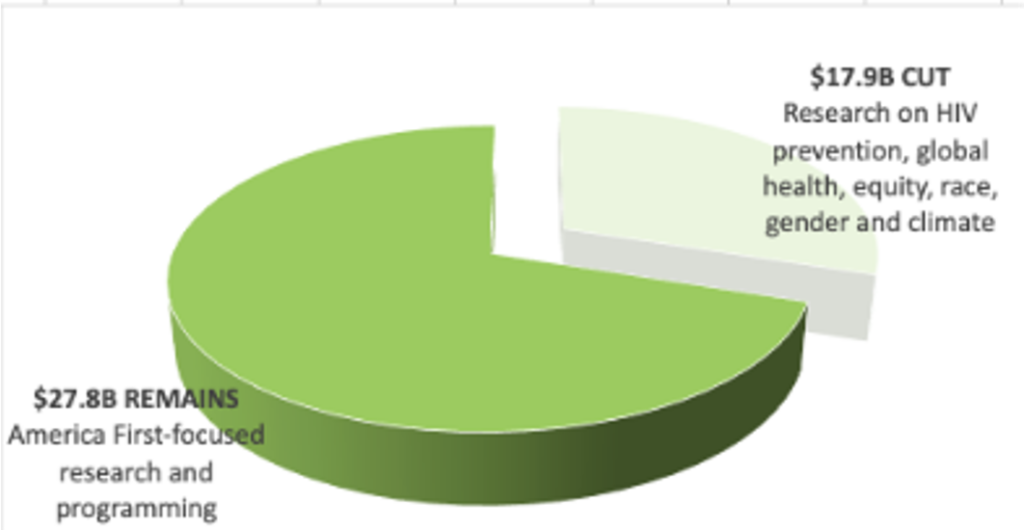
- Preserves $28 billion of the $46 billion for NIH overall, but excludes HIV prevention, global health, and health equity research.
- Reorganizes NIH into 5 “realigned” institutes, removing focus on climate, gender, racial equity.
- Eliminates the Fogarty International Center and the National Institute on Minority Health and Health Disparities.
Centers for Disease Control and Prevention (CDC): Cut by $3.59 billion
- Eliminates Global Health Center and National Centers on environmental health, injury prevention and chronic disease prevention.
- Eliminates DEI programs and shifts the burden for pandemic prevention and response.
Agency for Healthcare Research and Quality: Effectively eliminated
- Cited as redundant; targeted for work on climate and gender.
National Science Foundation (NSF): Cut by $4.9 billion (56%)
- Eliminates funding for work seen as ideologically objectionable (e.g., broadening participation and racial equity in STEM).
Global Health and Development
At a time when the USG should be expanding access to new technologies, the proposed FY26 budget guts foreign assistance funding, threatening pillars of the global HIV response: the President’s Emergency Plan for AIDS Relief (PEPFAR) and US contributions to multilateral initiatives, such as Global Fund and GAVI. The ideological targeting of family planning and gender-related programs will further weaken interventions to address HIV, which have been shown to work best within a comprehensive package of health and social services.

Global Health Programs: Cut by $6.23 billion
- Defunds NGOs providing family planning, impacting maternal and child health providers.
- PEPFAR preserved only for existing treatment programs and programs for the prevention of mother-to-child transmission (PMCT) , and specifically excludes primary prevention and PrEP, except for pregnant and lactating populations.
USAID Development Aid: Cut by $8.33 billion
- USAID is eliminated with the limited number of existing programs moved into the State Department.
- Eliminates DEI, climate, and gender-related programming.
- Creates new “America First Opportunity Fund” to replace foreign assistance grants with loans that prioritize US interests over humanitarian needs.
Centers for Disease Control and Prevention (CDC)
- STI, TB, hepatitis programs folded into a reduced $300 million block grant.
- For more on the specific impacts on STI programs, please read AVAC’s new brief on Worldwide Prevention, Shared Protection: Why STI Funding Matters.
Health Resources and Service Administrations (HRSA): Cut by $1.73 billion
- Ryan White HIV/AIDS Program activities not deemed core are eliminated.
Substance Abuse and Mental Health Services Administration (SAMSHA): Cut by $1.065 billion
- Eliminates harm reduction and regional substance use program grants.
Offices of Minority & Women’s Health
- Moved under a new, less visible structure.
New Initiative: “Make America Healthy Again”
- $500 million focused on lifestyle over treatment.
What This Means
- HIV Prevention R&D and global implementation is at risk. Cuts to NIH and USAID directly threaten support for clinical trials, community engagement, and biomedical innovation.
- Equity-centered research threatened. Eliminating institutes focused on minority and global health severely undermines inclusive science and jeopardizes future impact. Inclusion is not just a nice to have, it’s integral to achieving impact
- PEPFAR protections are narrow. Only existing beneficiaries are covered; scale up and innovation are excluded, compromising the imminent introduction and potential impact of injectable lenacapavir for PrEP. Funding for HIV prevention is also eliminated, except for pregnant and lactating populations.
Advocacy Priorities
- Monitor the full FY26 budget release for agency-level detail and justification.
- Engage Appropriations and other relevant Committees via coalition efforts (e.g., FAPP, GAPP, GHTC, SHF).
- Mobilize your community to contact your Senators and Representatives to let them know you oppose these cuts.
- Share your stories from researchers affected by cuts—particularly those whose work is globally focused or funded by NIH/USAID.
- Stay up to date with budget briefings and mobilization opportunities. See AVAC’s ‘Research Matters’ resource, which shares guidance and a toolkit for researchers to advocate for continued funding.
This budget is a threat to decades of progress in science, equity, and health—but it is also an opportunity to speak with clarity and urgency about what is at stake. Advocates must ensure that the future of HIV prevention, global health innovation, and equitable science is not written by politics, but by people, evidence, and impact.
Novel Study Designs for New HIV Prevention Products
A presentation by Deborah Donnell, of the Fred Hutchinson Cancer Research Center University of Washington, discussing trial design when PrEP is available. How can the field justify randomization to an experimental drug when we have something known to work? If we give study participants PrEP, how can we know a new experimental drug is working?
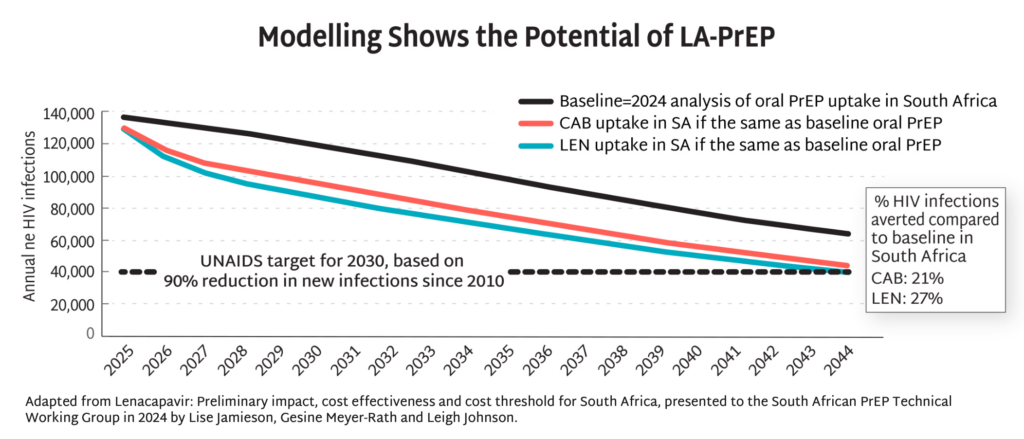
Modelling Shows the Potential of LA-PrEP
Modelling data from South Africa demonstrate the potential of injectable PrEP to dramatically reduce HIV incidence by up to 90% by 2044, and potentially even sooner with more aggressive uptake. This potential goes beyond South Africa, lighting the way toward epidemic control the world over. Excerpted from PxWire.
PxWire Volume 15, Issue 2
The field of HIV prevention is confronted with two opposing forces; programs for delivering PrEP have been shuttered all over the world by the withdrawal of the US government from global health. At this same moment in history, next-generation long-acting products hold great promise to accelerate HIV prevention and help the world achieve epidemic control. Navigating these seismic developments requires unprecedented coordination, solidarity, and courage.
Global health champions can defy the hatred, fear, and greed that are dominating politics in so many places around the world. Together we can innovate, create, and protect the advance of HIV prevention and global health. This issue provides a snapshot on threats to delivering PrEP, the potential of injectable lenacapavir (LEN) for PrEP, and on the implications of upstream research and development of other long-acting PrEP.
Read below or download the PDF version.
Progress in PrEP Uptake: Threatened
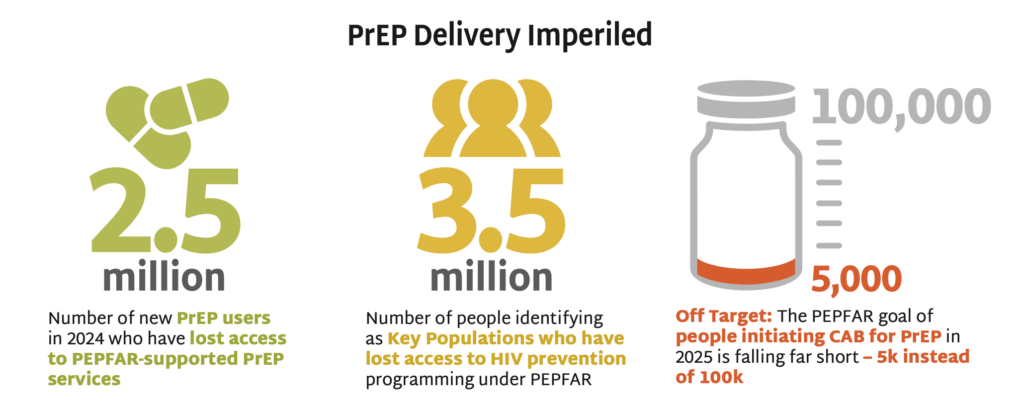
- PEPFAR documented 2.5 million new PrEP users in 2024, who could now lose access to PEPFAR- supported PrEP services. US Department of State issued a limited and inconsistently implemented waiver in February, allowing for continued provision of HIV treatment but restricting PrEP access to pregnant and lactating people only.
- These actions will result in 3.5 million who identify as key populations (KPs) losing access to all HIV prevention programming under PEPFAR, according to 2024 PEPFAR data tracking KP use of PrEP. These groups have higher rates of HIV incidence and face additional barriers to accessing services now that targeted programs are suspended.
- PEPFAR had a goal of 100,000 people initiating cabotegravir (CAB) for PrEP in 2025. But only 5,000 individuals had initiated by October 2024. The suspension of PEPFAR funding imperils scale-up of this long-acting product.
- These figures represent just some of the disruptions that are decimating PrEP delivery. Learn more here: Impact of PEPFAR Stop Work Orders on PrEP
- Overcoming this challenge, restoring, sustaining, and accelerating PrEP access is imperative and possible if the field works together.
For the last eight years, AVAC has proudly worked with PEPFAR to document PrEP uptake and its impact around the world. That stopped in January with a stop work order from the US government. But protecting access to PrEP is vital. Are you leading a PrEP program? Whether supported by PEPFAR or not, we invite you to work with us to ensure global data on PrEP is not lost. Find us at [email protected].
PrEParing for New Products
- Approval by the US Food and Drug Administration (FDA) for injectable 6-month LEN for PrEP is expected in June, with WHO guidelines expected in July. See the full timeline.
- Modelling data from South Africa demonstrate the potential of injectable PrEP to dramatically reduce HIV incidence by up to 90% by 2044, and potentially even sooner with more aggressive uptake. This potential goes beyond South Africa, lighting the way toward epidemic control the world over.
- The field must be prepared for swift action once LEN is approved and recommended, to ensure this opportunity is not squandered. As AVAC’s interactive timeline, Tracking LEN Rollout, outlines, donors, ministries of health, manufacturers, regulators, and civil society all have a role to play to pave the way for swift, equitable and effective introduction of LEN for PrEP.
The Latest R&D in the Prevention Pipeline
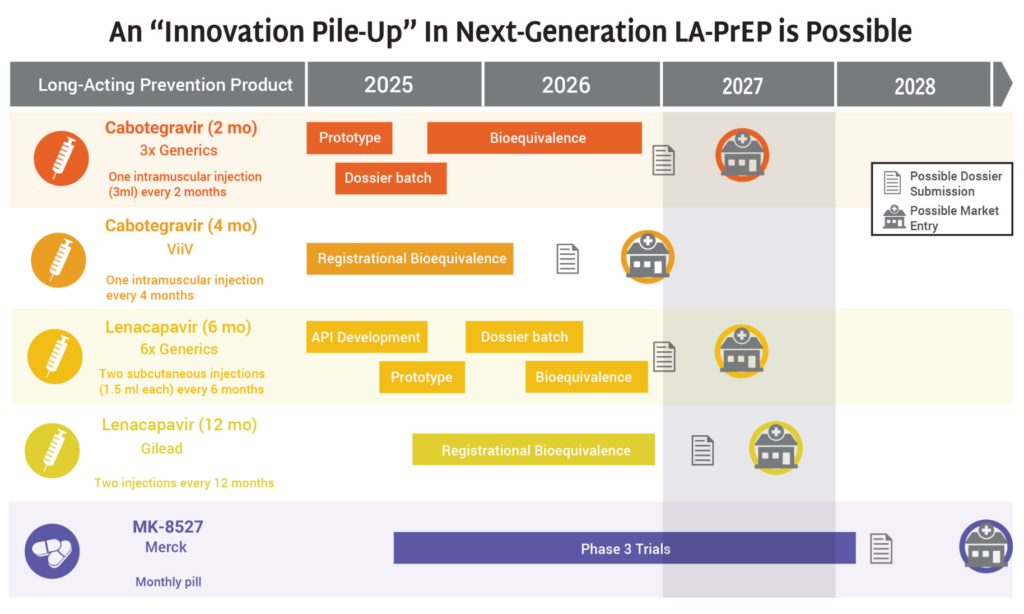
- The HIV prevention market is headed toward a period of significant opportunity—and possible congestion—as a slate of new products are on track for continued development and potential introduction to the market in 2027 and 2028.
- Generics for 2-month CAB and 6-month LEN, along with ViiV’s 4-month CAB, Gilead’s 12-month LEN, and Merck’s monthly oral MK-8527 PrEP pill (if further development and approvals are successful) could all enter the market by 2028.
- The possibility of so many products on the market, including four different formulations of injectable PrEP, means that it is imperative the field prepares for this future now.
- Markets and policies must be built to support the products in the market already, so that new options can be rapidly deployed and deliver impact. Otherwise, the field will squander time and money, with epidemic control slipping further out of reach.
- With US funding cuts to both HIV prevention R&D and delivery, communities must be engaged, supported, and informed about all prevention options, and the choices that all stakeholders will need to make. This means gathering and sharing data and information about cost-effectiveness, user acceptability, program feasibility, and impact. Communities empowered with the facts can advocate for the choices they need, and push ministries of health to make strategic investments and procure the prevention method mix that fits their context and delivers impact.
Prevention Playlist
AVAC develops a wide range of resources to inform decision making and action. Check out the latest:
Join
- Subscribe to Global Health Watch: AVAC’s weekly newsletter dedicated to breaking down critical developments in US policies and their impact on global health, at avac.org/global-health-watch
- CHANGE: In response to the unfolding crisis, more than 1,500 people from civil society organizations around the world have launched CHANGE—Community Health & HIV Advocate Navigating Global Emergencies—a coalition formed to support urgent action: [email protected]
Use
- Research Matters Advocacy Toolkit, AVAC
- Tracking the Freeze: Real-Time Impact on Key Populations, GBGMC
- Impact of the Stop-Work Order on PrEP, AVAC
- Tracking Lenacapavir Rollout, AVAC
- PEPFAR Program Impact Tracker, Impact Counter
- Weekly Situation Report, UNAIDS
Watch/Listen
- Politics and Global Health: The Need for a New, Resilient Architecture, Webinar
- Lawsuit Wins and What’s at Stake: AVAC v US Department of State, PxPulse episode
- Global Health in the Lurch: What’s happening now and who is pushing back, PxPulse episode
- Advancing Sexual and Reproductive Health and Rights: Moving forward post-the 2024 US Election, Webinar
Read
- Despite USG Global Health Collapse, Here Are Several Data Trackers To Support Your Advocacy, AVAC
- On Going Backwards, Lancet
- The Trump Administration’s Foreign Aid Review: Status of PEPFAR, KFF
- The Best Investment You Didn’t Know You Made: How NIH Funding Fuels Innovation and Economic Growth, amfAR
- HIV Market Impact Memo, CHAI
- The USAID List of Terminated Global Health Awards – What Does it Tell Us?, KFF
- AVAC Condemns HHS Mass Layoffs
- PrEP in the Balance: Hopes and fears in 2025
- Better Engagement, Better Evidence: Working in partnership with patients, the public, and communities in clinical trials with involvement in good participatory practice, Lancet
- PEPFAR: A Strategic Necessity for US Leadership and Global Health, AVAC
- Rallying for HIV Prevention Amid Policy Attacks, AVAC
- CROI 2025 Shows the Promise of Research at its Best, AVAC
The Role of PEPFAR in HIV Prevention
Protecting Black and Brown Communities Amidst Foreign Aid Cuts
AVAC Senior Program Manager for Policy, John Meade Jr., describes PEPFAR’s historic legacy and strongly argues for its continued importance in the face of attacks by the new US administration. This piece appears in The Broadsheet, the magazine published by the Congressional Black Caucus Health Braintrust.
Global Health in the Lurch: What’s happening now and who is pushing back?
KFF’s Jen Kates and AVAC’s John Meade break it all down on PxPulse Live.
A snapshot of global Health in the first weeks of the Trump Administration, this episode covers the impact of the US freeze on foreign aid to critical federal agencies and the HIV research pipeline and explores action in Congress and among civil society to push back.
Resources
Trials & Projects Halted by USAID Funding Suspension
The stop-work orders have disrupted USAID-supported HIV prevention research, halting critical investigations in vaccine and next-generation PrEP strategies.
The abrupt suspension of these trials also raises serious ethical concerns. Stopping trials mid-course undermines trust in research, jeopardizes community engagement, and abandons participants who volunteer their bodies for scientific discovery. It will take years to build back this critical infrastructure—for HIV research and beyond—as well as the community partnership and trust needed to ensure smooth and ethical research.