July 29, 2021
The field of HIV prevention research has two updated ethical guidance documents, one from the US National Institutes of Health-funded HIV Prevention Trials Network (HPTN) and the other jointly published by UNAIDS and WHO. Each of these documents updates prior versions, last published in 2009 for the HPTN and 2012 for UNAIDS/WHO. Here we explore the key similarities and differences in the two documents and their implications for the field.
Taken together, the HPTN’s Ethics Guidance for Research and UNAIDS/WHO’s Ethical Considerations in HIV prevention trials address the dominant issues in today’s world of HIV prevention research. They reflect the expanded array of prevention tools—including antiretroviral treatment as prevention for people living with HIV and a PrEP landscape that includes tenofovir-based oral PrEP today, with the Dapivirine Vaginal Ring (DVR) and injectable long-acting cabotegravir (CAB-LA)—and provide deeper guidance on critical decisions that come with trial operations and regulations.
The considerations and obligations put forward in these documents are not binding, but they are widely accepted by civil society, trial designers, product developers and researchers as crucial considerations for the design and execution of biomedical prevention trials.
The publications serve different primary audiences. The HPTN guidance is written specifically for the network’s researcher staff and partners and reflects US government policy and positions. The UNAIDS/WHO document is aimed at a global audience, including all research institutions as well as other decision-making bodies such as national ministries of health. Both set out principles that can be referenced by communities, researchers, policy makers, funders, regulators, and anyone engaging with a specific trial or with research overall.
In both cases, the authors were digesting major forces that affect HIV prevention research. The advent of oral PrEP, increasingly accessible since 2012, is making HIV prevention trials more complex. Participants must be offered this highly protective option—either in the “comparator” arm of a study where there’s no placebo, or as part of the standard package of prevention that participants receive when they are randomized to either a placebo product or an experimental one. (For more on issues in innovative trial design check out Bill Snow’s blog on AVAC, Designing a New Generation of HIV Prevention Efficacy Trials, and the May 2021 statement from the AVAC-convened Trial Design Academy on the future of HIV prevention trials.)
But providing PrEP involves a web of decisions about how to ethically fulfill this obligation, and how to design a trial that will be able to answer key questions in research. As new forms of PrEP move through the pipeline, this complexity will only grow. In addition, ethics bodies have been increasingly concerned with a number of other issues including: building lasting capacity to conduct research and respond to healthcare needs in the places where research takes place; addressing the social and political pressures faced by vulnerable populations as a factor in trial design; and expanding and deepening partnerships among host communities, populations that need prevention, and those who fund and conduct research.
Each of the 15 guidance points of HPTN’s Ethics Guidance for Research receives a designation as an “obligation” or an “aspiration” and names accountable entities, such as trial sponsors, researchers, community representatives, study teams and/or research sites.
Ethical Considerations in HIV prevention trials by UNAIDS/WHO tackles the ethics of trial design and conduct in 14 guidance points. Guidance Point 1 reasserts, in contemporary terms, why HIV prevention trials remain imperative. Despite the efficacy of PrEP and its increasing availability, transmission of HIV is outpacing current efforts to control the epidemic, and more choices for effective prevention are essential.
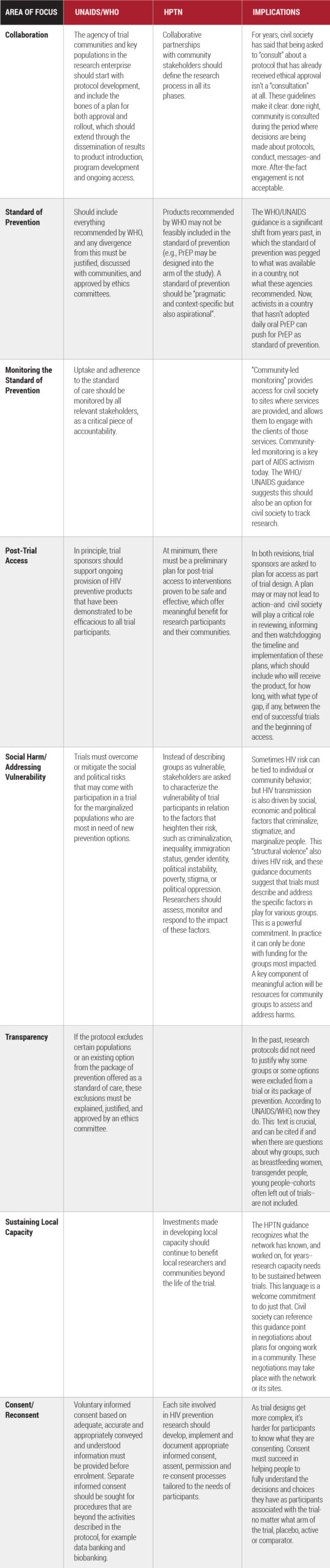
Many of the most significant changes in each publication echo each other, but there are some distinctions. This table (downloadable here) summarizes some of the key changes in both documents and their implications.
These two foundational documents set a standard that all HIV prevention stakeholders should seek to meet, and transparently. It’s important to note that they are intended and should be used as guides, not prescriptions. Where they leave off, the Good Participatory Practice Guidelines for biomedical HIV prevention trials (GPP) pick up. Developed by AVAC and UNAIDS, the GPP Guidelines look at how to involve stakeholders and build the partnerships that make research relevant and ensure results will lead to innovation that works for the people who need it. Researchers, sponsors, advocates, ministries of health, trial-site staff, regulators and anyone interested in HIV prevention research should know what’s in them all.