This infographic lays out AVAC’s top-line recommendations from AVAC Report 2019: Now What? The recommendations fall into three categories: deliver — prevention programs whose impact is well-measured and -defined; demonstrate — next-generation engagement for next-generation trials; develop — new targets for the post-2020 world.
AVAC’s “3D” View of the World: 2019 and beyond
A Generic and Unifying HIV Prevention Cascade Framework
What get’s measured matters if and only if that measurement is linked to impact. The most common approaches to evaluating primary prevention don’t measure up. They measure commodities but not use. A count of the condoms or PrEP bottles handed to people does not tell you whether the condoms were used, the pills were taken—or even, often, whether the people receiving the commodities were at high risk of HIV. A simple, universal prevention cascade could help change that. This one, which presumes that HIV testing has happened and is focused on people at risk of HIV, suggests four stages (see A) and then shows how solutions could be tailored to fix the cascade (see B).
Excerpted from AVAC Report 2019: Now What?
Visualizing Multisectoral Prevention: The DREAMS program theory of change
This is PEPFAR’s own visualization of how its AGYW programs can effect change. It’s notable for the definition of a care package that touches on the individual and her community, and for the way it defines a range of outcomes. There isn’t anything comparable for PEPFAR’s Key Population Investment Fund, which is infusing resources into a range of countries. Some of that funding is going for ART; for primary prevention, a theory of change linked to incidence is a must. AVAC is working with allies in KPIF countries to make this demand.
Excerpted from AVAC Report 2019: Now What?
AVAC Report 2019: With 2020 targets sure to be missed, we ask Now What?
Today, AVAC released Now What?, our 2019 annual report on the state of the HIV prevention field. Each year, the AVAC Report frames the most pressing advocacy issues facing the HIV response. At the threshold of 2020, it’s clear that global goals for HIV prevention will miss the mark by a long shot.
Though important progress has been made, the crisis UNAIDS called out in 2016 persists today with new infections around 1.7 million annually, a far cry from the 2020 target of fewer than 500,000.
So, we asked ourselves, Now What?, and answered with cross-cutting analysis and an advocacy agenda to match.
- Visit the Now What? website
- Download AVAC Report 2019: Now What?
- Download infographics from the Report
FIRST, we call for leadership that is bold, visible and activist, from the new head of UNAIDS, to houses of parliament to civil society coalitions: take uncompromising stances, demand accountability, speak out for intersectional issues of race, gender, class and climate. This work needs to be funded, full-throttle and fearless.
SECOND, we call for the use of today’s most recent evidence to guide new prevention targets that will pave the way for epidemic control. Clear milestones for the prevention research pipeline must be set. Investments over the past decades have provided us with the prevention options we have today, and much-needed new strategies are under now investigation. The field needs targets for prevention research that people can understand and influence.
THIRD, we call for multilayered prevention approaches that are centered around the person, not the virus. Since last World AIDS Day, we’ve learned again, perhaps most strikingly from the ECHO trial, about the dynamic needs of women for HIV and pregnancy prevention. The complexity of translating results into policy, bring renewed urgency to the need for comprehensive HIV prevention and reproductive health approaches. Multilayered prevention incorporates multipurpose strategies (i.e., products that prevent both pregnancy and HIV) within programs designed to address structural barriers (i.e., policy reform, transforming community norms, facilitating educational empowerment).
2020 will be a pivotal year—join us in calling on leaders, from the grassroots to global capitals, to make 2020 a turning point, when siloes come down, crises are transformed by innovation, and prevention is center stage in the fight against HIV.
Happy reading, and we’d love to hear how you answer Now What?
What’s New on AVAC.org and PrEPWatch.org
We don’t want you to miss a host of resources posted in recent weeks on AVAC.org and PrEPWatch. In case you missed them, these tools and resources will sharpen your take on the field.
Reporting on Global HIV Prevention
Check out these reports—recently published by AVAC and partners—for updates on funding trends in prevention and cure R&D, as well as a fresh look at places that have beaten back HIV with existing interventions:
- Translating Progress into Success to End the AIDS Epidemic offers an analysis of the interventions that succeeded in reducing HIV diagnoses and AIDS-related deaths in six places around world. The response in each location was tailored to its context and epidemic, but there are common elements that can be adapted anywhere.
- HIV Prevention Research & Development Investments: Investing to end the epidemic reports on overall 2018 investment in HIV prevention R&D and looks at funding trends. Findings include: 1.2 percent increased investment after five consecutive years of decline, investment in PrEP, female condoms and prevention of vertical transmission saw increases, while investment in voluntary medical male circumcision, preventive vaccines, microbicides, and treatment as prevention lost ground.
- Global Investment in HIV Cure Research and Development in 2018 estimates total funding for HIV cure-related research and looks at the drivers behind a 12 percent increase from 2017 to 2018.
Smarter Rollout
These articles and tools support advocates, implementers and decision-makers working on PrEP rollout today with an eye on future interventions tomorrow:
- Reaching and Targeting More Effectivley: The application of market segmentation to improve HIV prevention programmes, by AVAC’s Anabel Gomez and others, and published in the Journal of the International AIDS Society, explores how to leverage the power of market segmentation for the promotion and uptake of primary prevention.
- Just updated in July, AVAC’s Global PrEP Tracker on PrEPWatch.org provides the latest data on programs, number of enrollments by country, regulatory status and more.
- A User’s Guide to PrEP Tools offers a handy table to navigate the many tools produced by different organizations to support policy makers, implementers, providers and others on PrEP access, uptake and continuation. Use this table to learn more about these tools, who they’re designed for, and when to use them.
- The PrEP4Youth video series of public service announcements encourages adolescent girls and young women in South Africa to consider PrEP as an HIV prevention method. Created by the OPTIONS Consortium in collaboration with the South African National Department of Health, these videos feature popular actresses and put young women at the center with short empowering messages.
Apply to be an AVAC Fellow in 2020
AVAC would like to remind you that our call for applications for the 2020 class of AVAC Fellows is open until September 20. We encourage you to learn more about the program and share this information with your network!
An End to AIDS: A new report analyzing key prevention successes
AVAC is pleased to share a new report, Translating Progress into Success to End the AIDS Epidemic, produced in collaboration with amfAR and Friends of the Global Fight against AIDS, Tuberculosis and Malaria.
The report highlights six different places – London, Malawi, New South Wales, Rakai, San Francisco and Thailand – that have successfully reduced new HIV diagnoses and AIDS-related deaths through a combination of biomedical, policy, structural and rights-based interventions. The response in each location was tailored to its context and epidemic, but there are common elements that others can adapt to any context.
The report also includes a global timeline looking ahead to 2030, with “headlines of the future,” noting potential policy and research advances, as well as other social and structural changes that, based on current evidence, would directly impact progress on HIV.
Translating Progress into Success to End the AIDS Epidemic provides a roadmap for other cities, districts, states and countries to expand rights-based prevention and treatment today for immediate public health impact, while maintaining the long-term policy and research agendas for a sustainable end to the epidemic.
The bottom line is clear: Ending the epidemic is not simple anywhere, but possible everywhere.
The report was released today at a press conference at the IAS Conference on HIV Science 2019 in Mexico City with representatives from the collaboration. Link here for the press release announcing the publication of the report.
To learn more about the case studies and see a vision for a future where the end of the AIDS epidemic is within reach, you can find the full report at EndAIDS.org.
Press Release
The Future of the HIV Response
New report provides first-time analysis of success across six locations
Mexico City — For the first time, AIDS experts have brought together new assessments from six locations around the world that have made impressive progress fighting the epidemic, identifying the common contributors to success and providing a roadmap to ending the epidemic globally.
In a new report released today at IAS 2019 and on EndAIDS.org, amfAR, AVAC and Friends of the Global Fight Against AIDS, Tuberculosis and Malaria demonstrate how dramatic reductions in HIV incidence and mortality have been accomplished in six very different settings around the world: Thailand; Malawi; Rakai, Uganda; New South Wales, Australia; London, England; and San Francisco, United States.
The report provides a graph for each location, illustrating declining HIV rates and deaths, as well as policy decisions that drove advances against the epidemic. The report also maps out the future, showing how the required policy, structural and research advances can propel dramatic progress.
“This report highlights the reality that progress toward ending HIV shouldn’t be limited by geography or demographics,” Greg Millett, Vice President and Director of Public Policy at amfAR, said. “It also highlights how much easier we can achieve our goal by continuing to invest in scientific research, as well as policies that promote human rights.”
Common contributors to lowering HIV incidence and mortality across the six locations include:
- Campaigns to encourage HIV testing, particularly among groups that are most affected
- Free and easy access to treatment at the time of diagnosis with HIV
- Scale up of evidence-based HIV prevention, such as voluntary medical male circumcision, pre-exposure prophylaxis and harm reduction
- Concerted efforts to provide human rights-based services and social supports alongside programmes to fight stigma and discrimination
“There is nothing easy about achieving epidemic control, but in Malawi, a country with few resources, we have found that innovation and early adoption of new guidelines is key to rapid scale up of treatment and prevention,” said Maureen Luba, Africa Regional Advocacy Advisor for AVAC. “With 91% of people who are aware of their status on HIV treatment, Malawi is beginning to show progress on the way to ending the epidemic. But we can’t declare success too soon; we can’t step back now in Malawi or anywhere else.”
Chris Collins, President of Friends of the Global Fight Against AIDS, Tuberculosis and Malaria, said, “This report provides a new narrative. Ending the epidemic isn’t an insurmountable challenge but a question of putting the evidence to work and scaling access, particularly for those most at risk. It won’t be easy anywhere, but it is possible everywhere.”
The six locations profiled in the report were selected based on their progress in response to the epidemic and the availability of data and information about local policy interventions. The report authors also aimed to assess a mix of types of epidemics – some among key populations and others impacting broader populations.
“To eliminate HIV worldwide, we need not just great prevention tools, but also strategic and impactful investments and policies,” Adeeba Kamarulzaman, International AIDS Society President-Elect, said. “The report provides important new analysis of what has worked and what can be scaled to build on this success.”
###
About amfAR, The Foundation for AIDS Research: amfAR is one of the world’s leading non-profit organizations dedicated to the support of AIDS research, HIV prevention, treatment education and advocacy. Since 1985, amfAR has invested nearly US$550 million in its programmes and has awarded more than 3,300 grants to research teams worldwide. For more information, visit www.amfar.org.
About AVAC: Founded in 1995, AVAC is a non-profit organization that uses education, policy analysis, advocacy and a network of global collaborations to accelerate the ethical development and global delivery of AIDS vaccines, male circumcision, microbicides, PrEP and other emerging HIV prevention options as part of a comprehensive response to the pandemic. For more information, visit www.avac.org.
About Friends of the Global Fight Against AIDS, Tuberculosis and Malaria: Friends of the Global Fight Against AIDS, Tuberculosis and Malaria advocates for US support of the Global Fund and the goal to end the epidemics of AIDS, tuberculosis and malaria. For more information about Friends of the Global Fight, visit www.theglobalfight.org.
The International AIDS Society (IAS) leads collective action on every front of the global HIV response through its membership base, scientific authority and convening power. Founded in 1988, the IAS is the world’s largest association of HIV professionals, with members in more than 170 countries. Working with its members, the IAS advocates and drives urgent action to reduce the impact of HIV. The IAS is also the steward of the world’s most prestigious HIV conferences: the International AIDS Conference, the IAS Conference on HIV Science, and the HIV Research for Prevention Conference. For more information, visit www.iasociety.org.
The IAS Conference on HIV Science is the world’s most influential meeting on HIV research and its applications. This biennial conference presents the most critical advances in basic, clinical and operational research that moves science into policy and practice. Through its open and inclusive programme development, the meeting sets the gold standard of HIV research featuring highly diverse and cutting-edge studies. The 10th IAS Conference on HIV Science – known as IAS 2019 – is taking place in Mexico City, Mexico, on 21-24 July 2019. For more information, visit www.ias2019.org.
Activists on the Frontlines of the PEPFAR Planning Process: Week 1
Emily Bass is AVAC’s Director of Strategy & Content.
Every year, programs under the US Government’s President’s Emergency Plan for AIDS Relief (PEPFAR) make plans, set targets and define approaches for more than 50 countries around the world. This year, the process began on March 4, and will continue for three weeks in Johannesburg, with countries arriving in groups for the Regional Planning Meetings (RPM).
The first week wrapped up today, Friday, and AVAC was there along with partners from around the world, including strong representation from the Coalition to build Momentum, Power, Activism, Strategy and Solidarity in Africa, or COMPASS Africa, a unique North-South coalition focused on supporting data-driven activism and advocacy for impact in Malawi, Tanzania and Zimbabwe. Both Malawi and Tanzania were part of the first week’s planning meeting—so the impact of COMPASS was in full effect. With two more weeks to go in the planning process—and opportunities to input into the final Strategic Direction Summaries for the countries who have already met—here are some highlights to celebrate and issues to follow.
Negotiating National Policy Shifts is Possible—and Powerful
PEPFAR planning meetings focus on US government dollars, but the impact of those dollars depends on the policy environment in a given country. In recent years, more country government representatives have started to attend, creating an opportunity for decision-making about national policies and approaches that PEPFAR alone cannot control. In Tanzania and Malawi, COMPASS Africa partners included the Malawian Civil Society Advocacy Forum (CSAF), the Tanzanian DSDUT coalition and northern NGOs, AVAC, Health GAP, MPact, and amfAR.
Before the gathering, activists flagged a number of policy shifts that could improve impact and save lives in Tanzania, including moving from a pilot to a national program with PrEP; allowing HIV testing to be performed by frontline health workers, not just nurses; allowing multi-month ART prescriptions for up to six months for stable patients; and a clear Ministry of Health policy prohibiting forced anal exams for men suspected of being men who have sex with men (MSM). By the end of the week, the Government of Tanzania had agreed to all of these shifts, and Tanzanian civil society had been both bold and supportive in articulating the value of these approaches, a reminder that PEPFAR is not the only focus in these planning meetings. Country-level civil society has a crucial role to play in voicing the needs and priorities of people most at risk of and living with HIV, and using the moment to secure national policy shifts. Congratulations Team Tanzania!
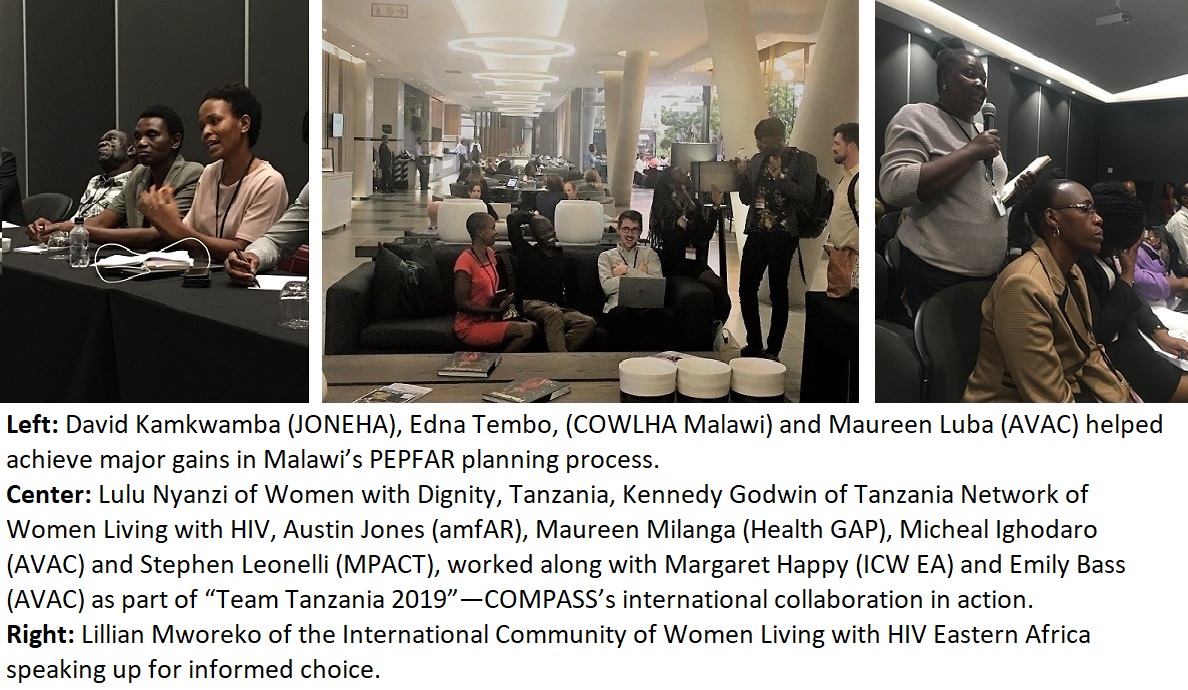
In Malawi, COMPASS partners from CSAF researched and drafted a “People’s COP”—part of the broader PEPFAR Watch project led by Health GAP, independent of COMPASS, in Kenya, Uganda and South Africa. AVAC’s Maureen Luba, the COMPASS regional Advocacy Advisor and a powerful member of Malawian civil society, worked alongside David Kamkwamba of the Network of Journalists Living with HIV and AIDS (JONEHA), chair of the CSAF, Edna Tembo of the Coalition of Women Living with HIV and AIDS (COWLHA), Health GAP’s Lotti Rutter and other civil society to advocate for demands based on the People’s COP. This potent coalition worked with government, the Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) and PEPFAR to negotiate many breakthroughs. These included a major shift in viral load monitoring, such that every PLHIV will now receive annual VL test and results. Other key wins included expansion of the program for voluntary medical male circumcision (VMMC) to three additional districts via a collaborative effort between GFATM and PEPFAR, investment in additional human resources for health, and funding for the scale-up of PrEP—a first in Malawi—to 10 districts in 2019-2020. Congratulations Team Malawi!
Getting Specific, Saving Lives: Civil society demands to protect informed choice and rights-based services for women and girls
Every country makes its own plans, but all receive some common marching orders from the US Office of the Global AIDS Coordinator, or OGAC. This year, these imperatives include accelerated rollout of dolutegravir (DTG)-based treatment regimens and ambitious scale-up of index testing, an approach that asks a person who’s tested HIV-positive (the “index” client) to provide the names and contact information of his or her biological children and sexual and needle-sharing partners, who are then followed up for testing. DTG leapt into the headlines earlier this year when a study from Botswana found a “safety signal” (an inconclusive but worrisome finding) that women who became pregnant while on DTG-based regimens were at slightly higher risk of a fetal abnormality known as neural tube defects (NTDs) compared to those taking efavirenz-based regimens. However, DTG is a well-tolerated drug with fewer side effects; people who take it achieve viral load suppression quickly and durably. In fact, at this week’s CROI conference, while PEPFAR negotiations were going on, South African scientists presented the finding that HIV-positive women who don’t start treatment until late pregnancy will reduce their viral load more quickly on DTG-containing regimens, making them less likely to pass HIV to their infants compared to women on efavirenz-containing regimens. (Check out our Twitter feed for a range of real-time CROI updates and stay tuned for an overview of the conference next week.)
The consensus, even before reaching Johannesburg, has been that DTG should be available to everyone who wants it, including women, in the context of contraceptive choices, and that index testing should be done with close attention to the impact on the index client, who might experience violence, stigma or “outing” as a sex worker, MSM or about his or her HIV status if the follow up is not done well.
For DTG, many countries, including Uganda, are adopting a written informed consent form that women must sign before starting the drug. In practice, this means many women aren’t receiving the medication because over-burdened health workers, who are also anxious about client’s health, may find it much easier to prescribe a regimen that seems less risky and doesn’t require a form. So, a step that’s supposed to protect women actually could put a needed drug further out of reach. As Lillian Mworeko, Executive Director of the International Community of Women Living with HIV Eastern Africa (ICW-EA) said, “Paper signing may be great, but it isn’t giving us what we need – what we are talking about is informed decision-making.”
AVAC and ICW-EA, a member of COMPASS, are longtime collaborators, and ICW-EA is supporting sexual and reproductive health advocacy across the region, along with other partners. Here is sample language that was developed this week, to consider adapting for inclusion in all 2019 PEPFAR Strategic Direction Summaries:
- On index testing: As part of the massive scale-up of index testing, PEPFAR [Country Name] will gather data on the results of the routine violence screening (conducted at every ART visit) for individuals who have submitted contact names, after those contacts have been traced, in order to identify increases in violence associated with index testing contact tracing. Specific attention to promoting and protecting the human rights of women and girls, along with key populations, is essential. Women often learn their HIV status before their male counterparts.
- On DTG transition: Initiation of DTG transition should start by date XX, be completed by XX, and include tracking of initiation by gender against the stated target [percentage of PLHIV to transition to DTG-containing regimens]. There should be real time review of whether there is gender parity in the percent of men and women transitioning to DTG regimens. If a gap emerges, with fewer women initiating, a rapid assessment of initiation procedures, including consent forms if utilized, should be undertaken. PEPFAR should also conduct assessment of % of ART sites that have FP on-site programmatically and that have stocks of contraceptives, tx/SRHR literacy investment to ensure there are expert clients (women) to do counseling on contraceptives and antiretroviral options. TLE to TLD transitioning should be coupled with treatment literacy led by the community. Women in child-bearing age should be given full information on benefits and risks of using DTG-based regimen and be given options to make informed decision and choice on whether or not be initiated on TLD. The rollout should be based on a human-rights based and woman-centered approach. Women who chose to remain on TLE should be given TLE 400mg for optimization.
Activists Need to Take on Testing: Here’s how!
Index testing isn’t the only hot topic in the arena of HIV testing. Recency testing—which can tell whether a person acquired HIV in the last six months—is also a focus of PEPFAR 2019, as is a rebalancing of testing approaches, or modalities, to emphasize “yield” (the number of people newly tested positive) and reduce costs. What gets counted is what matters. As AVAC has said for many years, a yield-focused approach risks omitting the needs of people who test HIV-negative, and who may be at risk. In addition, there are many questions about how to implement recency testing and to rebalance testing approaches in ways that achieve the desired aims. AVAC, amfAR and CHANGE together co-authored an issue brief on HIV testing strategies that PEPFAR has cited as a valuable guide to these issues—check it out and bring these concerns and questions into your PEPFAR country planning process.
Keep Watch on the Key Population Investment Fund
PEPFAR’s Key Population Investment Fund (KPIF) was first announced two and a half years ago. At the time, it was envisioned as a companion to the DREAMS Innovation Challenge, which would resource frontline groups to provide the services and spaces needed most for some of the groups hardest hit by the epidemic. This year brought the latest information on this long-awaited fund. The resources will flow, via USAID and CDC, directly to local organizations (if a pass-through is required, that organization won’t collect an overhead). What precisely will the funds be able to pay for? Here the language was finely-parsed and left some activists with questions. It is clear that the impact of the funds will be measured in terms of uptake of services, including HIV testing, and linkage to ART or PrEP. But the funds themselves can, PEPFAR says, be provided to groups that do things other than service delivery—such as supporting structural interventions like housing or human rights protections, that make it easier for people to test, choose biomedical strategies and remain in care. This is a tricky notion. Tying KPIF money to performance against PEPFAR indicators is a way of pushing back against what Ambassador Debbi Birx has called “feel good” programs that count people reached, without delineating what they received or what impact was had. (This refers to the KP_PREV indicator, which is poorly defined and deserves a closer look, as Ambassador Birx has acknowledged.) On the other hand, tying performance to these indicators could close space for frontline groups that do the essential work of keeping key and vulnerable populations alive and healthy, by combating injustices, stigma and human rights abuses or advocating around mental health concerns or education, as examples. AVAC and COMPASS partner MPact are actively monitoring the rollout of the newest iteration of the KPIF. We will be meeting with USAID and CDC to learn more in the coming weeks and months. Join us!
Want to learn more about how to inform PEPFAR—from in Johannesburg or afar? Check out these resources:
- MPact’s 2019 US PEPFAR COP Reviews: 10 tips for advocates – https://mpactglobal.org/2019-u-s-pepfar-cop-reviews-10-tips-for-advocates
- Health GAP’s PEPFAR Watch work includes collaborative “People’s COPs” and a roadmap to the PEPFAR process: https://healthgap.org/resources/pepfar-watch/
- amfAR has created user-friendly databases that allow activists to understand what’s happening with PEPFAR programming at the country level. Check out their database on performance (mer.amfar.org), which is part of the COMPASS initiative, and don’t miss amfAR’s database on country plans and budgets (copsdata.amfar.org). You can download country fact sheets in English, French and Portuguese.
Community Engagement and HIV Prevention Research
This December, Px Pulse features a gripping, tripartite conversation between activists Morenike Giwa-Onaiwu, Stacey Hannah and Jeremiah Johnson about what their long histories fighting for community engagement in HIV prevention research have taught them, and how these lessons can be applied today, and in the future. Tune in to hear three fierce voices with fresh perspectives on how to continue designing trials, and engaging communities, in today’s landscape of expanded, but inadequate, prevention choices.
With daily oral PrEP, VMMC, partner testing and treatment that leads to virologic suppression available as potent biomedical tools, along with condoms and a range of other structural interventions, clinical trials of biomedical HIV prevention strategies to block sexual transmission are more complex, in terms of design and conduct, than ever before.
Listen to this episode of Px Pulse on iTunes or at www.avac.org/px-pulse to learn why this conversation is at a critical moment and how to manage the opportunities for an innovative and collaborative effort with the research community.
Also, in case you missed it, check out the latest issue of Px Wire, which is hot off the presses. Our year-end edition offers 10 questions for activists to galvanize their work in the year ahead. We consider the future of NIH funding for HIV prevention and its research priorities, anticipated results from the ECHO trial, what’s next for the dapivirine ring and much more! The centerspread visualizes a single time frame for trial results and critical targets for incidence reduction and scale up of primary prevention-an essential perspective for the work ahead.
Finally, please don’t forget, your support makes our work possible. Help us continue with a year-end donation at www.avac.org/donate. You can also use smile.amazon.com for your online shopping and select AVAC as your charity of choice. A portion of your purchase price is donated to AVAC—at no additional cost to you!
Happy listening and reading, and happiest of holidays!
The Latest Issue of Px Wire! What to Watch in 2019
As 2018 winds down, we’re struck by the many moments, and movements, in the past year that have depended on listening, without bias and also without loss of conviction. From a bold activist challenge in an elevator, to an array of young women speaking their truths about HIV prevention—the future has hinged on being willing to listen, and on demanding to be heard.
In that spirit, our year-end edition of Px Wire offers 10 questions for activists to pose, with curiosity and conviction, in 2019. What answers do you want, what do you hear, what needs to happen next? We’ll be listening!
Our questions take on the upcoming announcement of how future NIH funding of HIV research will shape biomedical prevention, the anticipated results of the ECHO trial looking at how different contraceptive options impact women’s risk of HIV, the future of the dapivirine vaginal ring and much more.
In our centerspread, we provide a visual for uniting biomedical prevention research and implementation—a necessary fusion for our work in the coming year, and beyond.
Also necessary: your continued support. AVAC depends on your contributions of work, ideas and, yes, funds for our work! We appreciate your support in one or more of the following ways:
- Donate: Visit www.avac.org/donate.
- Amazon Smile: Shop at Amazon.com? Visit smile.amazon.com and select AVAC as your charity of choice and a portion of your purchase price is donated to AVAC—at no additional cost to you!
- US Combined Federal Campaign: If you are a US government employee, support our mission through the Combined Federal Campaign, CFC #12308.
Many thanks for your continued support, partnership and inspiration.