An Advocacy Chronicle on Universal Healthcare in Tanzania, with Atuswege Mwangomale of Sikika
In this episode of PxPulse: The Advocacy Chonicles, Atuswege Mwangomale goes deep on the advocacy work behind the passage of Tanzania’s Universal Healthcare Law. Atu serves as Head of Health Programs for Sikika, a Tanzania-based advocacy organization with a long track record of promoting best practices in governmental financing in the health sector, and advocating for improved health outcomes. Sikika, along with AVAC, is also a member of the COMPASS coalition, which uses data and coalitions across Africa to identify strategic campaigns to advance the HIV response.
Sikika’s advocacy has been crucial to the ultimate passage of Tanzania’s Universal Health Insurance Bill in 2023, but full funding must still be secured for the law to achieve full impact.
Atu explains the promise of UHC in Tanzania, how Sikika won the trust of government allies, and why working in coalition was essential to success.
A Year in the Life of GPP: What’s actually happening, and how do we know it’s working?
The Good Participatory Practice (GPP) Guidelines have been shaping and improving HIV prevention research since 2007. They provide a global reference guide for ethical and effective stakeholder engagement, helping ensure the priorities of trial participants and their communities are centered in clinical trials and broader research agendas.
One year ago, AVAC published the Good Participatory Practice (GPP) Body of Evidence, an online clearinghouse of tools, best practices and analyses showcasing the power of GPP. Here, we bring you a report from the year since – how this clearinghouse of resources continues to demonstrate the value of GPP, and concrete examples from 2024 of GPP’s impact on major research agendas and mechanisms. Read on for highlights.
Critical Learnings from GPP: The Body of Evidence Webinar Series
Throughout 2024, AVAC and partners facilitated a series of webinars in collaboration with The Global Health Network, Wellcome Trust, and WHOfeaturing resources housed in the Body of Evidence. These conversations expanded the traditional understanding of GPP – highlighting that GPP is not just about trial implementation; that its practices evolve from product discovery to delivery and are important at every step of the way; and that monitoring and evaluation are complex and critical nuances are required to ensure its meaningful application. Look out for a final webinar on elevation of GPP in global clinical trials guidance in 2025. The full recordings and presentations are on the AVAC website.
Our great leader Nelson Mandela said, ‘everything that is done for me, without me, is done against me,’ and we really must see our community members as having a role beyond that of as just a potential trial participant but to engage them right from the beginning, from the protocol design, from all our planning pre-study, the conduct of the study, and most important to the dissemination of the results – whether they be positive or negative. — Dr. Michelle Temeris, University of Capetown
How can we craft research questions so that when we have an answer at the end of the day it’s really something meaningful and impactful to communities? We can answer scientific questions that might be interesting to a researcher but at the end of the day that doesn’t get us very far if it’s not also equally impactful for community. — Sarah Read, US National Institute of Allergy and Infectious Diseases
Thinking about community engagement moving forward we need to think about building relationships over time and beyond particular studies. We need to make sure that we’re not only giving accurate information but we’re also listening and responding to issues that are being raised in the course of our interactions. —Sassy Molyneux, KEMRI-Wellcome Trust, University of Oxford
One really important perspective would be to monitor the impact that engagement has on the trial, the way it’s run. That would be a really important aspect of monitoring and evaluation – to make note of the real changes that community stakeholders can have on the way trials are selected in the first place but also modified to make them appropriate. — Alun Davies, Global Health Network
GPP in Action: Influencing Research Programs
Advocates’ Consultation on Merck’s Monthly Pill Program
In recent years HIV prevention efficacy trial design has become one of the hottest topics. As the HIV prevention toolbox improves, researchers, statisticians, and regulators grapple with the best way to incorporate these options into efficacy trials. The key to all of this, they say? Community.
Enter GPP! In June, AVAC convened a community and advocates’ consultation with Merck around their program testing MK-8527 as a monthly pill for PrEP. With an efficacy program on the horizon, Merck set out to consult with communities – before any other stakeholder – about issues like choice of a comparator arm, the evolving standard of prevention, and how a trial could best reflect the reality of implementation in peoples’ countries, communities, and own lives. Consultation members consolidated feedback that is now being fed into Merck’s protocol development. Priorities included a design that would get to an efficacy answer most efficiently, but that would incorporate contextual issues of prevention choice as possible. Participants concluded that a monthly pill would be an important addition to the prevention toolkit, and thus support for the research program. But they also expressed ongoing frustration around community support for research that does not translate into access for their communities.
Watch this space for further updates on the MK-8527 program, as engagement continues through protocol development, trial planning, implementation, and beyond!
Pediatric Adolescent Virus Elimination (PAVE) Community Advisory Board (CAB)
Communities have been a key stakeholder advancing HIV cure research from the bench to early phase clinical trials. GPP has been the guiding principle as engagement has moved further upstream.
The Pediatric Adolescent Virus Elimination (PAVE) Community Advisory Board (CAB) is an example of this impact as the only group dedicated to advancing an HIV cure in pediatric populations. Through its digital Voices Project featuring young people with HIV, clinicians, caregivers and researchers, the CAB has raised awareness of the research among youth in Sub-Saharan Africa who engaged with ministries of health to push for the inclusion of children in research. They also worked with PAVE investigators to simplify and convey complex scientific and ethical issues inherent in cure research.
As research moves from the bench to the clinic, the CAB and community partners, will continue to play a strategic role in shaping future protocol designs and addressing community support needs.
Since AVAC and UNAIDS launched the GPP guidelines in 2007, the science and politics have grown ever more complex – and GPP implementers have continued to adapt, evolve and engage. We are committed to continuing our efforts to curate insights and resources, including further building out the Body of Evidence, and to support our collective advocacy for ethical and effective stakeholder engagement throughout clinical trials, research agendas and implementation in the months and years to come.
Moving a Product to the “Real World”
A visual roadmap illustrating the key stages transitioning a product from clinical trials to large-scale real-world implementation.
PxPulse: The Votes are In — What’s next for the US’ role in global health and HIV prevention
In the days, months and years ahead under a new US Presidential Administration, advocacy for choice, freedom, science, and rights will require intentional strategies to protect hard fought gains in HIV treatment and prevention and in global health generally, and to safeguard policies and programs that advance it. And there will be major implications for the global AIDS response.
Navigating through the work ahead involves assessing the potential impact on PEPFAR and Global Fund support; on USAID, NIH, CDC and the FDA; on the US relationship to WHO and other UN agencies; and on evidence- and rights-based policies and programs generally. Joining us to begin those efforts and better understand the landscape for advocacy are Jen Kates from KFF and our own Suraj Madoori.
This Week at AVAC: US election, new LEN resources, STI pipeline and PrEP service delivery
As we continue to grapple with the results of the US presidential election and what this means for our work and for global health evidence- and rights-based policies and programs generally, we wanted to share a range of new tools and resources you may find helpful in your advocacy for choice, science and rights.
The past few months have brought exciting developments in the field of Sexually Transmitted Infections (STIs). The World Health Organization released the global priorities for STIs, which included the need to develop low-cost, rapid, STI point-of-care tests, vaccines, and communication strategies to increase STI awareness, prevention, service engagement. But we continue to see a soaring rise in STI incidence and an underfunded infrastructure for researching new treatment, prevention and testing tools. It’s up to the global community to ensure that research and development continues to see funding for better, faster, less expensive tools to reduce the toll of STIs. Read on for resources and insights to guide your advocacy.
Conference updates
The annual conference of the International AIDS Society in July highlighted the troubling trend in the soaring rise in STI incidence. A preconference, Mobilize for Action on Sexually Transmitted Infections addressed the urgent need to confront the global spike in STI rates, particularly syphilis, gonorrhea, chlamydia, and trichomoniasis. Dr. Jeanne Marrazzo, director of NIAID, when discussing the number of global deaths from syphilis, which is treatable, said, “I think some of the more staggering statistics here, in addition to the sheer number of new infections, is the fact that we had in 2022 over 200,000 syphilis-associated deaths, which to me is practically medieval.” The meeting hosted a rigorous debate exploring the question of implementing DoxyPEP, given there’s no efficacy data for cisgender women in light of fears of creating drug resistant strains of STIs from wider use of doxycycline. Strong arguments were made on both sides, but this controversy is one of the reasons AVAC recently published an Advocate’s Guide to Doxycycline to Prevent STIs.
The STI Prevention Conferencein Atlanta, Georgia convened attendees in-person for the first time in four years and discussed the rise in syphilis rates, emerging gonorrhea treatments, STI funding and policy initiatives, and doxycycline post-exposure prophylaxis (DoxyPEP). Notably, much discussion centered on NIAID’s support for a biorepository to advance diagnostic development. This biorepository would streamline access to necessary specimens to support the research and development of new diagnostics.
Save the date
New resources
Discover STIWatch.org!
STIWatch.org is an updated platform designed to enhance understanding and advocacy for STI vaccine and diagnostics research, development, and rollout. It offers comprehensive information on common STIs, a clinical trials dashboard, advocacy priorities, and a range of resources and tools to support STI prevention and treatment efforts.
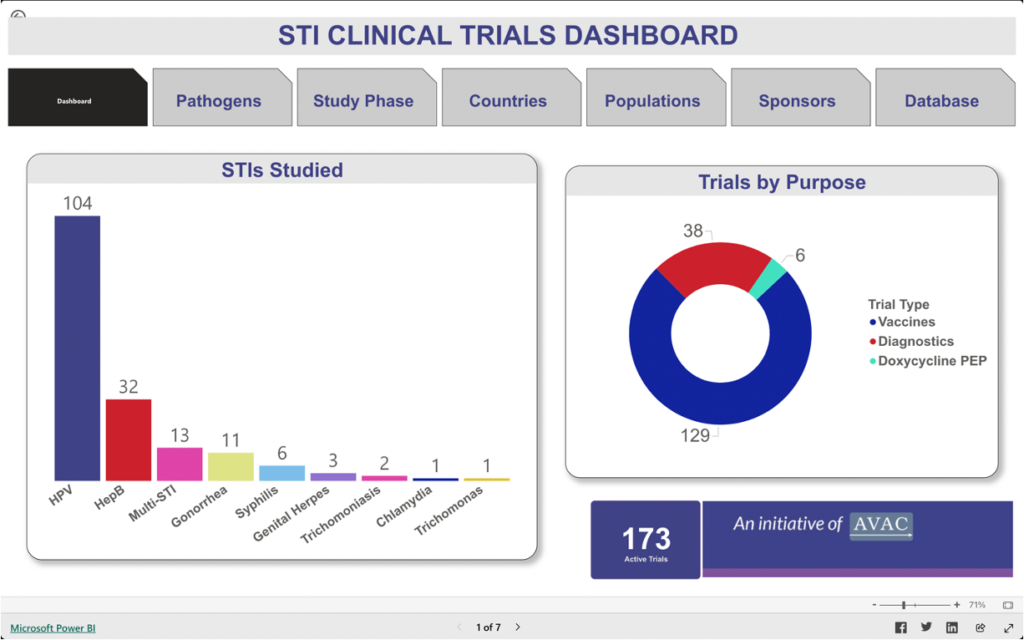
STI Clinical Trials Dashboard
This dashboard provides information about trials focused on vaccines, diagnostics, and the use of doxycycline post-exposure prophylaxis (DoxyPEP) to detect, treat, and prevent chlamydia, gonorrhea, hepatitis B, herpes simplex virus (HSV), human papillomavirus, syphilis, trichomoniasis infections, and Mycoplasma genitalium.
Webinar Summary
Regulatory Pathways to Promote Access to STI Diagnostics. This webinar co-hosted with World Health Organization (WHO) supported researchers, product developers and the global advocacy community in identifying and discussing ways to bring new STI diagnostics to market with speed, equity and scale.
What We’re Reading
Special Issue: Sexually Transmitted Diseases. This leading journal celebrated 50 years by publishing a series of editorials that review the careers of some of the leading experts in the field. These stories are both inspiring and enlightening, highlighting the decades of efforts and growth in addressing STIs. AVAC’s own, Alison Footman, PhD, wrote about her experiences in the STI field and how instrumental mentorship has been in her career growth.
Gonorrhea point-of-care diagnostics technology and market landscape. This landscape report provides an overview of gonorrhea point-of-care diagnostics that can be offered closer to patients and communities and limit time to results and ultimately treatment. Gonorrhea touches on multiple public health priorities including the need to reduce STI rates, growing antimicrobial resistance, and its impact on sexual and reproductive outcomes and HIV transmission.
FDA Marketing Authorization Enables Increased Access to First Step of Syphilis Diagnosis. The US Food and Drug Administration approved the first syphilis self-test. This is a monumental step in expanding syphilis testing options as infections have increased drastically over the past five years. Self-tests can provide people with the option to learn their syphilis status and seek additional testing and treatment options from a healthcare provider.
Partner Spotlight
AVAC partners have been busy moving the needle to improve STI prevention, testing, and treatment options in their respective countries. The Latu Human Rights Foundation partnered with HEP Initiative Zambia on a symposium to foster ideas on how to better address viral hepatitis and integrate hepatitis B interventions into other government funded health programs.
To learn more about AVAC’s STI Program, visit STIWatch.org and avac.org/sti. Email sti@avac.org for questions or additional information. And to sign up for specific updates on STIs, click here.
STIWatch Newsletter, November 2024
The past few months have brought exciting developments in the field of Sexually Transmitted Infections (STIs). The World Health Organization released the global priorities for STIs, which included the need to develop low-cost, rapid, STI point-of-care tests, vaccines, and communication strategies to increase STI awareness, prevention, service engagement. But we continue to see a soaring rise in STI incidence and an underfunded infrastructure for researching new treatment, prevention and testing tools. It’s up to the global community to ensure that research and development continues to see funding for better, faster, less expensive tools to reduce the toll of STIs. Read on for resources and insights to guide your advocacy.
Conference updates
The annual conference of the International AIDS Society in July highlighted the troubling trend in the soaring rise in STI incidence. A preconference, Mobilize for Action on Sexually Transmitted Infections addressed the urgent need to confront the global spike in STI rates, particularly syphilis, gonorrhea, chlamydia, and trichomoniasis. Dr. Jeanne Marrazzo, director of NIAID, when discussing the number of global deaths from syphilis, which is treatable, said, “I think some of the more staggering statistics here, in addition to the sheer number of new infections, is the fact that we had in 2022 over 200,000 syphilis-associated deaths, which to me is practically medieval.” The meeting hosted a rigorous debate exploring the question of implementing DoxyPEP, given there’s no efficacy data for cisgender women in light of fears of creating drug resistant strains of STIs from wider use of doxycycline. Strong arguments were made on both sides, but this controversy is one of the reasons AVAC recently published an Advocate’s Guide to Doxycycline to Prevent STIs.
The STI Prevention Conferencein Atlanta, Georgia convened attendees in-person for the first time in four years and discussed the rise in syphilis rates, emerging gonorrhea treatments, STI funding and policy initiatives, and doxycycline post-exposure prophylaxis (DoxyPEP). Notably, much discussion centered on NIAID’s support for a biorepository to advance diagnostic development. This biorepository would streamline access to necessary specimens to support the research and development of new diagnostics.
Save the date
New resources
Discover STIWatch.org!
STIWatch.org is an updated platform designed to enhance understanding and advocacy for STI vaccine and diagnostics research, development, and rollout. It offers comprehensive information on common STIs, a clinical trials dashboard, advocacy priorities, and a range of resources and tools to support STI prevention and treatment efforts.
STI Clinical Trials Dashboard
This dashboard provides information about trials focused on vaccines, diagnostics, and the use of doxycycline post-exposure prophylaxis (DoxyPEP) to detect, treat, and prevent chlamydia, gonorrhea, hepatitis B, herpes simplex virus (HSV), human papillomavirus, syphilis, trichomoniasis infections, and Mycoplasma genitalium.
Webinar Summary
Regulatory Pathways to Promote Access to STI Diagnostics. This webinar co-hosted with World Health Organization (WHO) supported researchers, product developers and the global advocacy community in identifying and discussing ways to bring new STI diagnostics to market with speed, equity and scale.
What We’re Reading
Special Issue: Sexually Transmitted Diseases. This leading journal celebrated 50 years by publishing a series of editorials that review the careers of some of the leading experts in the field. These stories are both inspiring and enlightening, highlighting the decades of efforts and growth in addressing STIs. AVAC’s own, Alison Footman, PhD, wrote about her experiences in the STI field and how instrumental mentorship has been in her career growth.
Gonorrhea point-of-care diagnostics technology and market landscape. This landscape report provides an overview of gonorrhea point-of-care diagnostics that can be offered closer to patients and communities and limit time to results and ultimately treatment. Gonorrhea touches on multiple public health priorities including the need to reduce STI rates, growing antimicrobial resistance, and its impact on sexual and reproductive outcomes and HIV transmission.
FDA Marketing Authorization Enables Increased Access to First Step of Syphilis Diagnosis. The US Food and Drug Administration approved the first syphilis self-test. This is a monumental step in expanding syphilis testing options as infections have increased drastically over the past five years. Self-tests can provide people with the option to learn their syphilis status and seek additional testing and treatment options from a healthcare provider.
Partner Spotlight
AVAC partners have been busy moving the needle to improve STI prevention, testing, and treatment options in their respective countries. The Latu Human Rights Foundation partnered with HEP Initiative Zambia on a symposium to foster ideas on how to better address viral hepatitis and integrate hepatitis B interventions into other government funded health programs.
To learn more about AVAC’s STI Program, visit STIWatch.org and avac.org/sti. Email sti@avac.org for questions or additional information. And to sign up for specific updates on STIs, click here.
Avac Event
Update on Injectable Lenacapavir for PrEP
AVAC hosted a webinar focused on updates for the PURPOSE trials for injectable lenacapavir for PrEP. Gilead provided an overview of the PURPOSE 1 and 2 trial results and insight into the status of PURPOSE 3, 4, and 5. This was be an opportunity for civil society to hear from Gilead directly.
People’s Research Agenda
Community & Advocacy Priorities in HIV Prevention Research Development
Led by AVAC alongside a network of partners, the People’s Research Agenda puts forward recommendations to diversify and strengthen the HIV prevention pipeline, enhance investment and financial support for HIV prevention research and development, and guide an advocacy strategy that truly addresses the needs of communities across the prevention pipeline.
The PRA is a living document developed through intentional consultative processes that used multiple modalities, including surveys, focus groups, convenings, to gather insights about the processes and products needed to actualize HIV prevention justice.
In this summary of the People’s Research Agenda, you’ll find the PRA’s core insights into the processes involved in HIV prevention research and implementation, and the types of products that should be developed through these processes.
The 5th HIV Research for Prevention (R4P) conferenceis being held in Lima, Peru from 6 to 10 October. Held every two years, HIVR4P is the only global conference to focused exclusively on biomedical HIV prevention, including AIDS vaccines, microbicides, PrEP, treatment as prevention and other approaches.
See below for conference highlights, recaps and announcements.

 Enter GPP! In June, AVAC convened a community and advocates’ consultation with Merck around their program testing MK-8527 as a monthly pill for PrEP. With an efficacy program on the horizon, Merck set out to consult with communities – before any other stakeholder – about issues like choice of a comparator arm, the evolving standard of prevention, and how a trial could best reflect the reality of implementation in peoples’ countries, communities, and own lives. Consultation members consolidated feedback that is now being fed into Merck’s protocol development. Priorities included a design that would get to an efficacy answer most efficiently, but that would incorporate contextual issues of prevention choice as possible. Participants concluded that a monthly pill would be an important addition to the prevention toolkit, and thus support for the research program. But they also expressed ongoing frustration around community support for research that does not translate into access for their communities.
Enter GPP! In June, AVAC convened a community and advocates’ consultation with Merck around their program testing MK-8527 as a monthly pill for PrEP. With an efficacy program on the horizon, Merck set out to consult with communities – before any other stakeholder – about issues like choice of a comparator arm, the evolving standard of prevention, and how a trial could best reflect the reality of implementation in peoples’ countries, communities, and own lives. Consultation members consolidated feedback that is now being fed into Merck’s protocol development. Priorities included a design that would get to an efficacy answer most efficiently, but that would incorporate contextual issues of prevention choice as possible. Participants concluded that a monthly pill would be an important addition to the prevention toolkit, and thus support for the research program. But they also expressed ongoing frustration around community support for research that does not translate into access for their communities.