PrEPWatch is designed to be a clearinghouse for information on PrEP research (ongoing and completed; clinical trials and demonstration projects), data, additional research, cost, access and advocacy efforts across the globe.
PrEPWatch
Px Wire July-September 2022, Vol. 12, No. 2
PrEP Tracker data, preparing for new products, the HIV prevention pipeline and our prevention playlist. All that and more in the latest issue of Px Wire.
Webinar Roundup — Including An Upcoming Webinar With Tony Fauci!
In October AVAC’s calendar of webinars took on a range of topics, each crucial for the field, and November’s webinars will be just as rich and diverse. Read on for highlights from October’s discussions and related resources, and be sure to register for webinars and events that are coming up this month, including a Fireside Chat with Tony Fauci!
Upcoming Webinars and Meetings
PEP Needs Some Pep! Addressing PEP Neglect in HIV Prevention Research, Programming and Uptake
Thursday, November 3 at 9:00am ET; 16h00 EAT
Register here
PEP, post-exposure-prophylaxis, is an HIV prevention intervention marked by both great promise and profound neglect. PEP works, but far too few people know about, or when and how to obtain this valuable intervention. Join The Choice Agenda for a discussion with James Ayieko, Julie Fox, Ken Mayer, Catherine Koss, Njambi Njuguna and Ace Robinson.
Africa Health R&D Week 2022
November 8 – 11, 2022, virtual
Register here
Join AVAC, IAVI, CASPR and others for a continental forum on domestic resource mobilization (DRM) for health research and development (R&D) in Africa. This week-long program for advocates, media, policymakers, program implementers, researchers, and funders will bring clarity to key issues and trends of DRM for health R&D in Africa.
Agenda / Concept Note / Flyers
Reintroducing PrEPWatch
Thursday, November 10 at 9:00am EDT; 17h00 EAT
Register here
Join us as we introduce AVAC’s updated PrEPWatch.org, a one-stop clearinghouse for the latest PrEP data on implementation and uptake, resources, and information on PrEP policies, programs and products, approved and in development. During this webinar, we’ll share:
- New data on PrEP rollout worldwide and by country.
- New ways to access global and country-specific PrEP resources for PrEP planning and advocacy.
- Stories of innovation from the field.
- Toolkits for each phase of planning, from policies & budgets to monitoring & evaluation, and everything in between.
Much Accomplished, Much to Do: A Conversation Looking Back & Looking Ahead with Tony Fauci
Monday, November 28 at 11:30am EDT; 18h30 EAT
Register here
Join AVAC for a conversation with NIAID Director, Anthony Fauci as we discuss all that’s been accomplished in the HIV and COVID-19 responses over the years, what’s ahead, and what the future looks like for NIAID, for Dr. Fauci and for pandemic preparedness.
Recordings and Resources
Doxycycline for STI prevention: Evidence and Current Research
Featuring Dr. Connie Celum, Jennifer Mahn, Dr. Victor Omollo, Rodney Perkins and Dr. Jenell Stewart
Recording / Slides / Resources
Private Sector Delivery Opportunities for the Dual Prevention Pill (DPP): Lessons from family planning (FP) for the introduction of multi-purpose prevention technologies (MPTs)
Co-hosted by AVAC and FP2030, this webinar highlighted findings from a report on private sector opportunities for the DPP and explored lessons from the family planning field
Recording / Slides / Resources
RINGing the Bell for Choice: Actions and Solutions on Dapivirine Ring (DVR) Access
The Choice Agenda hosted a conversation around the latest in DVR advocacy last month. Watch the webinar, explore up-to-date resources on DVR, and sign-up for The Choice Agenda listserv—a growing community of over 800 prevention advocates and counting.
RINGing the Bell for Choice: Actions and Solutions on Dapivirine Ring Access
Thursday, September 22, 2022
Hear the latest updates from African advocates leading the advocacy for access to the dapivirine ring. Plus tune in for the Population Council’s plans for moving the ring forward on multiple fronts, from roll-out of the monthly ring to research around the 3-month ring and multipurpose ring.
AVAC Condemns Court Decision that Tramples Human Rights, Reinforces Homophobia and Denies Life-Saving PrEP Drugs to Individuals in Texas
As a global organization dedicated to health as a human right, to social justice, and to individual autonomy and choice, AVAC condemns the decision by a federal judge in Texas who ruled in favor of a historically homophobic, misogynistic, and discriminatory plaintiff. A conservative activist sued on behalf of a Texas company claiming that adhering to a provision of the Affordable Care Act requiring employers to provide coverage for HIV pre-exposure prophylaxis (PrEP) drugs violates their religious rights.
“This shocking ruling defies evidence, logic, public health and human rights and sets back enormous progress made in the fight to end the HIV epidemic in the US and globally,” said Mitchell Warren, AVAC’s executive director. “It is a blatantly homophobic and misogynistic ruling that will endanger the lives of many gay men and others who rely on PrEP to protect themselves from HIV.”
“This ruling is the latest blow in a campaign to roll back bodily autonomy and human rights for a wide swathe of the American people. The Supreme Court overturning of Roe v. Wade earlier this year was a wake-up call that individual rights are under attack by the far right,” Warren added. “This decision likely won’t be the last we see in a campaign to impose some individuals’ religious beliefs on the broader population. Access to contraception, vaccinations, routine health screenings, prevention services and patient privacy are all under attack.”
While this latest decision is for now limited to the Northern District of Texas, it has ramifications for the rest of the country and for global programs to provide PrEP to people of all genders and sexual orientations who need and want to use it. These kinds of decisions often test the ground for cases that go to the Supreme Court, where the current makeup of the court means such a decision may be upheld and even expanded upon nationally.
“Deciding to use PrEP is a decision between an individual and their healthcare provider, no one else. Another person’s religious beliefs have no place in determining the right to use a safe, highly effective, FDA-approved, life-saving drug,” said Suraj Madoori, AVAC’s director of policy and advocacy.
“Daily oral PrEP was approved by the US FDA a decade ago and still has not reached nearly all of those who would benefit from its use. This decision throws up another substantial barrier between a life-saving intervention and individuals and communities most vulnerable to HIV, further capping the untapped potential of an important prevention option,” Madoori added.
This decision creates enormous, unnecessary barriers for LGBTQ+ people in Texas, as well as heterosexual women who are HIV-vulnerable, from the healthcare they need and is yet another example of oppressive or criminalizing policies in countries around the world that set barriers to health and human rights. We know these barriers drive poverty, epidemics and disenfranchisement from civil society. Policies like this don’t advance anyone’s freedom to live full, healthy lives; rather they undermine community resilience, individual autonomy and public health.
“At a time when science has given us the tools to advance towards the end the HIV epidemic and rational evidence-based public health policies and programs can implement those tools to save millions of lives around the world, one judge’s biased and discriminatory decision could endanger programs and lives far beyond northern Texas,” Warren added. “As advocates, activists and citizens, we at AVAC stand in solidarity with those whom this decision affects. We firmly believe that the ruling must be called out as homophobic and dangerous and that every effort must be made to ensure that it does not stand.”
###
About AVAC: Founded in 1995, AVAC is a non-profit organization that uses education, policy analysis, advocacy and a network of global collaborations to accelerate the ethical development and global delivery of HIV prevention options as part of a comprehensive response to the pandemic. Follow AVAC on Twitter @HIVpxresearch and find more at www.avac.org and www.prepwatch.org.
Press Release
AVAC Condemns Court Decision that Tramples Human Rights, Reinforces Homophobia and Denies Life-Saving PrEP Drugs to Individuals in Texas
As a global organization dedicated to health as a human right, to social justice, and to individual autonomy and choice, AVAC condemns the decision by a federal judge in Texas who ruled in favor of a historically homophobic, misogynistic, and discriminatory plaintiff. A conservative activist sued on behalf of a Texas company claiming that adhering to a provision of the Affordable Care Act requiring employers to provide coverage for HIV pre-exposure prophylaxis (PrEP) drugs violates their religious rights.
“This shocking ruling defies evidence, logic, public health and human rights and sets back enormous progress made in the fight to end the HIV epidemic in the US and globally,” said Mitchell Warren, AVAC’s executive director. “It is a blatantly homophobic and misogynistic ruling that will endanger the lives of many gay men and others who rely on PrEP to protect themselves from HIV.”
“This ruling is the latest blow in a campaign to roll back bodily autonomy and human rights for a wide swathe of the American people. The Supreme Court overturning of Roe v. Wade earlier this year was a wake-up call that individual rights are under attack by the far right,” Warren added. “This decision likely won’t be the last we see in a campaign to impose some individuals’ religious beliefs on the broader population. Access to contraception, vaccinations, routine health screenings, prevention services and patient privacy are all under attack.”
While this latest decision is for now limited to the Northern District of Texas, it has ramifications for the rest of the country and for global programs to provide PrEP to people of all genders and sexual orientations who need and want to use it. These kinds of decisions often test the ground for cases that go to the Supreme Court, where the current makeup of the court means such a decision may be upheld and even expanded upon nationally.
“Deciding to use PrEP is a decision between an individual and their healthcare provider, no one else. Another person’s religious beliefs have no place in determining the right to use a safe, highly effective, FDA-approved, life-saving drug,” said Suraj Madoori, AVAC’s director of policy and advocacy.
“Daily oral PrEP was approved by the US FDA a decade ago and still has not reached nearly all of those who would benefit from its use. This decision throws up another substantial barrier between a life-saving intervention and individuals and communities most vulnerable to HIV, further capping the untapped potential of an important prevention option,” Madoori added.
This decision creates enormous, unnecessary barriers for LGBTQ+ people in Texas, as well as heterosexual women who are HIV-vulnerable, from the healthcare they need and is yet another example of oppressive or criminalizing policies in countries around the world that set barriers to health and human rights. We know these barriers drive poverty, epidemics and disenfranchisement from civil society. Policies like this don’t advance anyone’s freedom to live full, healthy lives; rather they undermine community resilience, individual autonomy and public health.
“At a time when science has given us the tools to advance towards the end the HIV epidemic and rational evidence-based public health policies and programs can implement those tools to save millions of lives around the world, one judge’s biased and discriminatory decision could endanger programs and lives far beyond northern Texas,” Warren added. “As advocates, activists and citizens, we at AVAC stand in solidarity with those whom this decision affects. We firmly believe that the ruling must be called out as homophobic and dangerous and that every effort must be made to ensure that it does not stand.”
###
About AVAC: Founded in 1995, AVAC is a non-profit organization that uses education, policy analysis, advocacy and a network of global collaborations to accelerate the ethical development and global delivery of HIV prevention options as part of a comprehensive response to the pandemic. Follow AVAC on Twitter @HIVpxresearch and find more at www.avac.org and www.prepwatch.org.
Upcoming TCA Webinars On CROI And The Ring!
The Choice Agenda, a global forum for advocacy on the latest in HIV prevention, has two webinars coming up you won’t want to miss:
![]()
CROI and Community and YOU – Preparing for CROI 2023
Wednesday, September 7 at 10:00-11:00am ET; 2:00-3:00pm GMT
Join the conversation with co-chairs of the Conference on Retroviruses and Opportunistic Infections (CROI), as well as researchers, advocates, community educators and members of the Community Liaison Subcommittee. The discussion will touch on what to expect at CROI 2023, which features some of the most consequential research on HIV, monkeypox, SARS-CoV-2 and more. The webinar will also cover how to apply for a Community Scholarship, and key dates and deadlines for engaging with the conference. Remarks from:
- Dawn Averitt, Member of the Community Liaison Subcommittee
- Dr. James Hoxie, Chair of the 2023 CROI Planning Committee
- Drs. Diane Havlir, Vice-Chair of the 2023 CROI Planning Committee
- Landon Myer, Vice-Chair of the 2023 CROI Planning Committee
- Jim Pickett, Member of the Community Liaison Subcommittee
- Ntando Yola, Member of the Community Liaison Subcommittee
RINGing the bell for Choice: Actions and Solutions on Dapivirine Ring Access
Thursday, September 22 at 9:00-10:30am ET; 1:00-2:30pm GMT
This webinar will offer the latest from African advocates leading efforts to demand access to the dapivirine vaginal ring. In recent weeks, advocates have been pressing PEPFAR and others to do more to deliver the ring to women who want it. The Population Council will also discuss their plans for moving forward a full agenda for ring technology, including rolling out the approved monthly PrEP Ring, and continuing research on a three-month ring and multipurpose technology. In July, the Population Council announced it had acquired the ring technologies from the International Partnership for Microbicides, the ring’s developer. Speakers include:
- Yvette Raphael, Advocacy for Prevention of HIV and AIDS, South Africa
- Leonard Solai, IPM, South Africa
- Erica Gollub, Pace University
- Chris Obermeyer, The Global Fund
For previous webinars from The Choice Agenda, check out our archive here! And join more than 600 advocates on the TCA listserve by reaching out to Jim at [email protected].
For Your Advocacy – A Research Agenda for Pregnant and Lactating People
For prevention options to meet the real life circumstances of the people who need them, we need an inclusive research agenda. Advocacy for the inclusion of pregnant and lactating populations (PLP) in research has been gaining traction in recent years, building on growing evidence, several global and national initiatives and an increased focus from prevention advocates. AIDS 2022 in Montreal featured exciting discussions advancing this work. If you’ve been taking part or just getting up to speed on the issue, AVAC has resources for you—including An Advocate’s Guide to Research in Pregnant and Lactating Populations; a dedicated page on AVAC.org with background and further resources; and a four-point action plan, Advancing HIV Prevention Research in Pregnant and Lactating Populations: Priority Advocacy objectives and Next Steps.
Pregnancy and the post-partum period after giving birth are times of heightened HIV risk. Cisgender women are two to three times more likely to acquire HIV during pregnancy and four times more likely post-partum than otherwise. Women who acquire HIV during pregnancy have an 18 percent chance of transmitting HIV to their newborn, which goes up to a 27 percent chance if they acquire HIV while breastfeeding. But HIV prevention options for (PLP) are limited, and their inclusion in research has been inadequate, resulting in evidence gaps across the research landscape for new prevention products.

(Image from AVAC’s Advocates Guide)
An approach based on principles of reproductive justice is reframing the research agenda for PLP. But action is needed from a variety of stakeholders to promote ethical inclusion rather than exclusion of pregnant people from clinical trials. A multi-stakeholder think tank led by AVAC and the PHASES project brought together advocates, researchers, ethicists, regulators and donors and resulted in a four point action plan, with additional contributions from Pangaea Zimbabwe AIDS Trust. The plan identifies next steps and four priority goals:
1) Embrace a reproductive justice framework:

(Reproductive Rights Framework, Image from PHASES, 2020)
2) Engage stakeholders in an early and sustained process in the design and conduct of clinical trials
3) Develop the necessary regulations to generate needed data for PLP to safely use new therapeutics
4) Ensure sound ethics reviews that include adolescent girls and young women in HIV prevention research.
An inclusive research agenda for PLP is essential for the HIV response, elemental to equity in global health, and key to having an impact on the epidemic. If you are interested in getting involved in AVAC’s work in this area, contact [email protected]
For other resources toward an inclusive research agenda, check out
- The Choice Agenda list serve: a global forum for advocacy on the latest in HIV prevention research, with monthly webinars on the hottest topics.
- No Data No More: A Manifesto to Align HIV Prevention Research with Trans and Gender-Diverse Realities
- Good Participatory Practice Guidelines: systematic guidance on effective stakeholder engagement in HIV prevention research.
Px Wire April-June 2022, Vol. 12, No. 1
Newly relaunched, PxWire is AVAC’s quarterly update covering the latest in the field of biomedical HIV prevention research and development, implementation and advocacy. Download for a quick look at where we are in HIV prevention.
New Issue of PxWire!
PxWire is AVAC’s quarterly update covering the latest in the field of biomedical HIV prevention research and development, implementation and advocacy. Each issue includes news, emerging issues and features upcoming events.
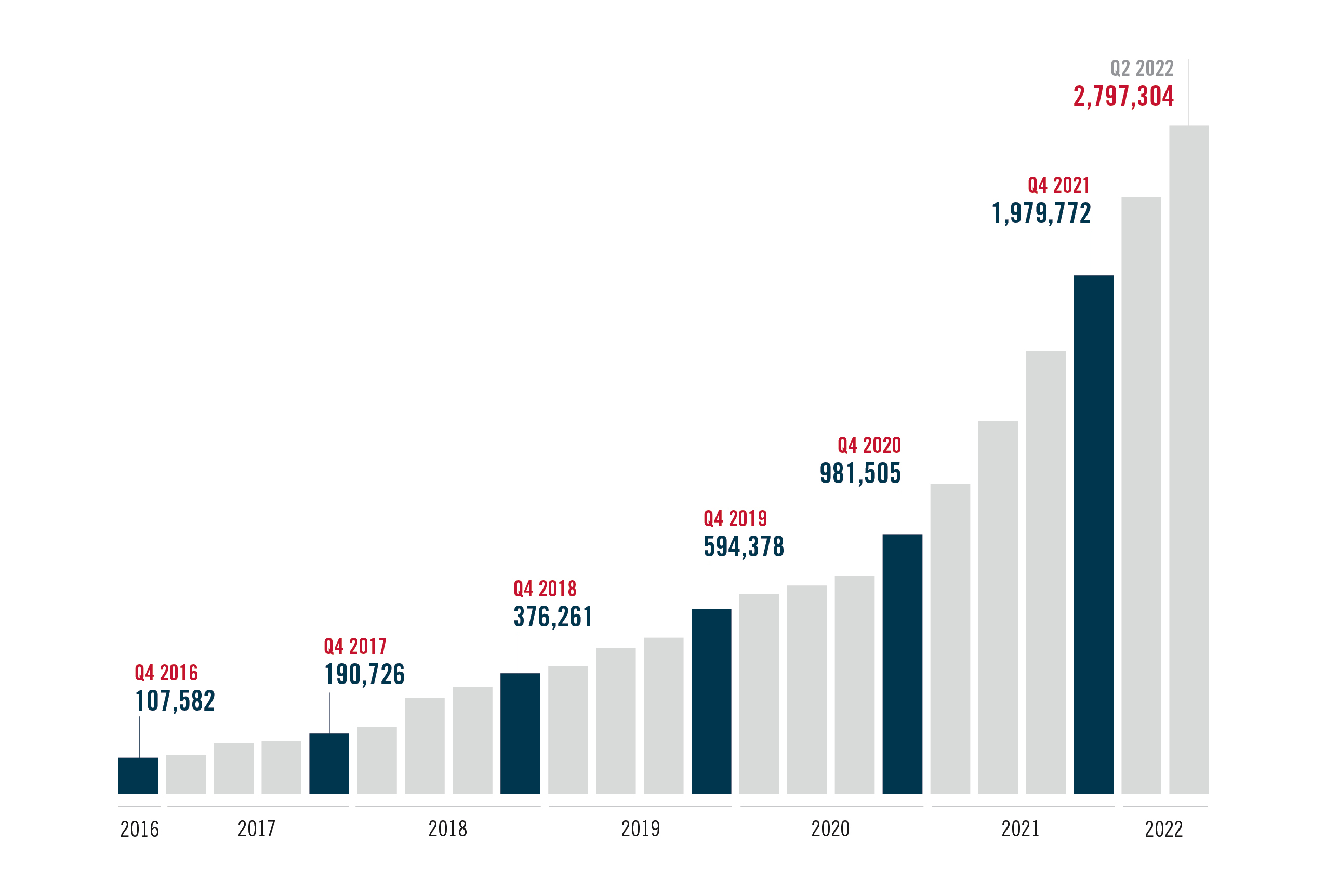
The HIV field gathers for its first hybrid International AIDS Conference (IAC) since the start of COVID-19 pandemic at a pivotal moment in HIV prevention. Across research to rollout – accelerated product access, new products reaching the market, new trials starting (and pausing) and recent research results – the ability to deliver two new proven PrEP methods will be determined by conversations and decisions happening now.
After initial approval ten years ago, oral PrEP initiations have surpassed 2M globally, reaching 2,797,304 – with significant progress over the past year, but still well below UN targets.
Check out the full issue of PxWire here and scroll down for important updates.