AVAC calls for intensified efforts to increase access to daily oral PrEP
AVAC welcomes new, additional data that shows an injectable antiretroviral for HIV pre-exposure prophylaxis (PrEP) is safe and highly effective in reducing HIV risk cisgender men and transgender women who have sex with men. At the 23rd International AIDS Conference today researchers from the HIV Prevention Trials Network (HPTN) released data comparing rates of HIV among trial participants who received the bi-monthly injection, and those who received daily oral tenofovir/emtricitabine (TDF/FTC). While both strategies reduced HIV risk among participants, the injectable strategy was more effective compared to oral PrEP.
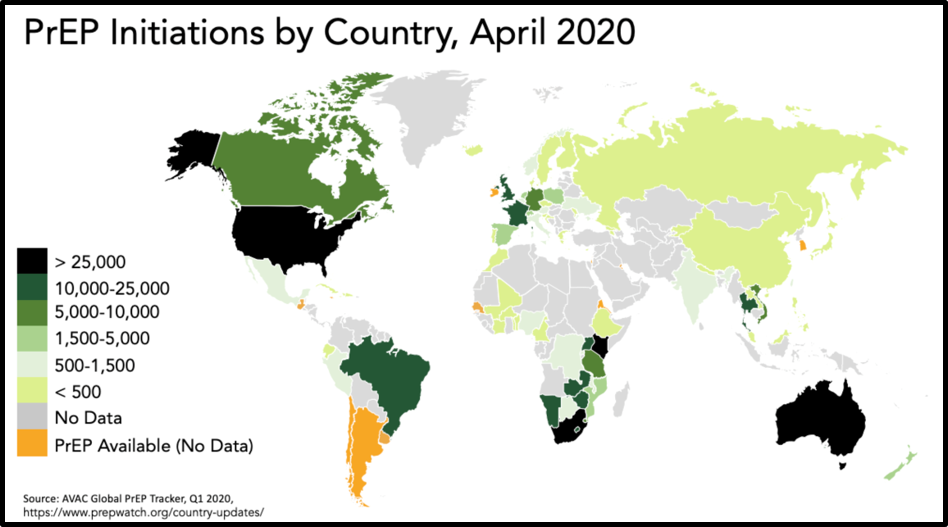
The overall number of infections in both arms of the study was very low, underscoring the high efficacy of both interventions. Importantly, daily oral PrEP is licensed and available now for men, women and adolescents in many communities around the world.
“It’s great to see such a high level of efficacy in a potential additional HIV prevention option and to see the high level of efficacy for an already available option, daily oral PrEP,” said Mitchell Warren, AVAC Executive Director. “As we celebrate this exciting new data, we also must ensure that the companion HPTN 084 study of the same product in cisgender women finishes as quickly as possible and simultaneously work to ensure broader access and support for daily oral PrEP in communities where it is needed now.”
These data add insight to the May 2020 announcement from HPTN 083 that injectable PrEP was highly-effective. Importantly, investigators shared data on adherence among participants taking oral PrEP and found that 76 percent of a random sample had blood levels consistent with daily use. While additional work to understand the results is ongoing, this suggests that the difference in impact might be due to the products. Use of the injection requires an oral “lead-in” phase, and 48 weeks of oral PrEP use after discontinuation. Learning more about preferences and feasibility of both injectable and oral PrEP among people at risk of HIV is a critical next step.
“We need options that will work in people’s lives, we need existing daily PrEP delivered at scale now, and we need multiple additional PrEP options to address diverse needs. CAB-LA, the dapivirine vaginal ring, and future products that show efficacy must be brought to market as quickly as possible,” added Warren.
Given that current data show efficacy in men who have sex with men and transgender women, but not in cisgender women, where rates in adolescent girls and young women are persistently high, messages, licensure and introduction plans need to be swift, clear and strategic with respect to the growing array of PrEP options available for different groups. ViiV, the manufacturer of CAB-LA, must now move quickly to work with regulatory agencies, to share, for community review and input, its plans for seeking review and the timeline for incorporating data from the ongoing HPTN 084 study, while WHO must simultaneously launch a parallel consultative process to support guidance for CAB-LA, so there will be no delay in rolling the drug out.
In 2018, AVAC and the Clinton Health Access Initiative (CHAI) established the Biomedical Prevention Implementation Collaborative (BioPIC) to work with a wide range of stakeholders to develop an introduction plan for long-acting injectables and other next-generation HIV prevention options. Today’s announcement makes planning all the more important if promising research results are to be translated into public health impact.
“Planning for health systems to meet future demands for a drug delivered by injection every two months must also be prioritized,” said Jessica Rodrigues, AVAC’s Director of Product Introduction and Access. “Daily oral PrEP was proven effective more than a decade ago, yet people who want and need this vital prevention option are still unable to access it in many communities. We must not repeat that cycle with new prevention options like CAB-LA and the monthly dapivirine vaginal ring for women, which is currently under regulatory review.”
These clinical trials are an important step in the process, but much additional work is needed. Every product has unique attributes and challenges, and there is much more to be understood about CAB-LA and the way in which it might be effectively delivered in communities and among populations where it is most needed. The HPTN 083 team is still analyzing the safety data on the oral lead-in period as well as the potential need for oral PrEP to “cover the tail” of participants who wish to stop receiving CAB-LA. The research to date suggests that stopping CAB-LA and clearing the drug from the body may not be as easy as stopping daily oral PrEP, since traces of CAB-LA can linger in the body well after discontinuing injections. It will be essential to understand how this can be addressed outside of a clinical trial setting.
“Understanding the potential risk of drug resistance, user preferences, health system capacity needs, the price of the product and the programs to deliver it and support use, amongst other issues, are necessary to move forward as quickly as possible if the product is ultimately approved for use,” said Rodrigues. “AVAC and our partners have already begun this work and have valuable insights; it now needs to accelerate with global collaboration so that the delays that have slowed the rollout of daily oral PrEP do not recur again.”
Also at AIDS 2020, the SEARCH study presented additional information on the impact of oral PrEP in the context of a comprehensive “health-fair” based approach. SEARCH previously found that this approach, which provided ‘universal testing’ and same-day antiretroviral treatment, reduced incidence by about 30 percent. In the latest data, the SEARCH team found that once daily-oral PrEP was offered to SEARCH participants, new HIV infections dropped by about 75 percent, compared to the period when PrEP was not yet available. This underscores the feasibility and urgency of making oral PrEP a part of comprehensive programs, anchored in a universal testing approach.
“The UNAIDS report and much of the news at this conference is reminding us that the world was failing at HIV prevention before the COVID-19 pandemic hit. SEARCH shows us the possibilities for PrEP success in some of the hardest hit communities in East Africa,” Warren said. “It’s critical that we find ways to scale up innovative daily oral PrEP programs even as we plan for access to new HIV prevention options. We can’t afford any more delays.”