In 2017, reported funding for HIV prevention R&D decreased by 3.5 percent (US$40 million) from the previous year, falling to US$1.13 billion. The full report, HIV Prevention Research & Development Investments 2017: Investing to end the epidemic, is available for download. And all the graphics are available as well.
Global HIV Prevention R&D Investment by Technology Category, 2000-2017
HIV Prevention R&D Trial Participants by Region in 2017
Participation of volunteers and the engagement of communities in which trials take place is essential to conducting HIV prevention research. In 2017, there were nearly 600,000 participants in HIV prevention research trials globally, mostly originating from sub-Saharan Africa, Europe, North America and Asia. A majority of participants were enrolled in research investigating TasP and PrEP, and while there are trials aimed specifically at men who have sex with men (MSM), transgender individuals and people who inject drugs, most of the studies do not specify the need to include members of key populations.
The full report, HIV Prevention Research & Development Investments 2017: Investing to end the epidemic, is available for download.
Investment in HIV Prevention R&D by Top Philanthropic Funders in 2017
Global philanthropic funding increased by 4.1 percent from 2016 levels and amounted to US$164 million, or 14.6 percent of overall funding. The Bill and Melinda Gates Foundation (BMGF) remained the largest funder and increased its contribution by 6.6 percent, to US$150.2 million. Wellcome Trust investment fell for the fifth consecutive year to an annual US$2 million.
The full report, HIV Prevention Research & Development Investments 2017: Investing to end the epidemic, is available for download.
Prevention Research Funding Report 2017: Investment slows and continues to concentrate in a few funders!
[UPDATE]: The new report was a feature story by UNAIDS, Global HIV prevention targets at risk.
Today, the Resource Tracking for HIV Prevention R&D Working Group (Working Group) launched its 14th annual report—which details 2017 investments—at the HIV Research for Prevention (HIVR4P) conference in Madrid.
Flat and/or reduced funding for HIV/AIDS and other global health issues threatens to roll back progress worldwide. There is belated and widespread acknowledgment of a prevention crisis that can only be addressed by taking today’s tools to scale while researching new ones. Given this backdrop, the report is a powerful advocacy tool. This year’s report notes troubling trends in investment flows for biomedical HIV prevention at a moment of major promise in the research landscape. The report tracks the origins, trends and direction of global funding as well as the resulting effect(s) on the prevention research funding landscape.
- Download HIV Prevention Research & Development Investments, 2017: Investing to end the epidemic
- Download graphics from the report
- Download the press release
Key Findings
The report shows that funding for HIV prevention research funding declined for the fifth consecutive year—and by 3.5 percent in 2017 to US$1.13 billion—the lowest total observed since 2005. This reduction was unevenly distributed. Investment increased for pre-exposure prophylaxis (PrEP) and voluntary medical male circumcision (VMMC) but decreased for AIDS vaccines, microbicides, prevention of vertical transmission (PMTCT), treatment as prevention (TasP) and female condoms.
The overall decline is driven largely by a reduction in US public-sector funding, with levels dropping by 5.8 percent from 2016 to US$830 million. This is a five-year low in investment. Outside the US public sector, another major decrease came from the European Commission, with funding levels dropping by 47 percent to US$7.6 million in 2017. The impact of these cuts was cushioned by increases from Australia, Brazil, Canada, Japan and the Netherlands. While the number of philanthropic donors decreased from 12 to 10 in 2017, levels of funding grew by 4.1 percent to US$164 million or 14.6 percent of overall funding. This is largely due to the 6.6 percent increase in investment from the Bill & Melinda Gates Foundation.
The report notes that the HIV prevention R&D space is at an exciting yet precarious juncture. Ongoing late-stage efficacy trials for preventive AIDS vaccines, long-acting injectable PrEP and antibody-mediated prevention could yield new options in the coming years. Then there’s also the dapivirine vaginal ring that is currently awaiting a regulatory opinion from the European Medical Association. However, the current funding landscape is not set up for sustainability or longevity, which is essential to help ensure that new products move from research and eventually to those who need it. Out of every dollar spent on HIV prevention research, 87 cents are from the two biggest donors, the US public sector and the Gates Foundation—a literal case of having all the coins in one basket. The report advocates for diversifying the funding base and developing long-term funding strategies to support the delivery of innovative prevention tools and a durable end to the epidemic.
The Resource Tracking Working Group hopes these reports will serve as tools for advocacy and be used to inform public policy that supports and helps to accelerate scientific progress. We thank all of the individuals who contributed data to the report and who gave time and effort as trial participants.
Check out the report, share it with your fellow advocates, and be sure to let us know if your organization is a funder or recipient of HIV prevention grants, or if you have further questions!
We are kicking off the launch of the report with a press conference at HIV R4P, which can be viewed live at the conference Facebook page and will be archived on the conference website.
Press Release
Continued declines in HIV research funding put global prevention targets at great risk
Contacts
AVAC: Kay Marshall, [email protected], +1-347-249-6375
IAVI: Anita Kawatra, [email protected], +1 212-847-1055
Madrid – HIV prevention research funding continued to decline in 2017 for the fifth consecutive year, driven largely by a five-year low in US public sector funding, according to a report released today at the HIV Research for Prevention (HIVR4P 2018) conference in Madrid, Spain.
The Resource Tracking for HIV Prevention R&D Working Group’s 14th annual report, Investing to End the Epidemic, documents funding that fell to the lowest level in more than a decade: In 2017, funding for HIV prevention research and development (R&D) decreased by 3.5 percent (US$40 million) from the previous year, falling to US$1.13 billion.
This declining funding comes at a time of great optimism for research, with a slate of efficacy trials across the prevention pipeline – including major HIV vaccine, passive antibody and next generation PrEP efficacy trials – and critical follow-on research for proven antiretroviral-based prevention options, notably the dapivirine vaginal ring. But it also comes a time when the broader HIV field is grappling with a prevention crisis that is exacerbated by decreased funding for the overall HIV response and a lack of political will to adequately fund a response that will ensure the world meets the ambitious prevention targets to end the epidemic.
The Working Group warns that getting to zero new infections will not only require the expansion of existing options like voluntary medical male circumcision (VMMC) and oral pre-exposure prophylaxis (PrEP), but also the development of innovative new products, including long-acting, antiretroviral-based prevention options and a vaccine. Sustained funding is critical to keep the full gamut of HIV prevention research moving forward in a timely manner. Even small declines in funding can delay or sideline promising, new HIV prevention options that are needed to end the HIV epidemic.
“Make no mistake. We are in a prevention crisis and we cannot afford a further funding crisis,” said Mitchell Warren, AVAC executive director. “It is unacceptable that donor funding for HIV prevention research continues to fall year after year even as research is moving new options closer to reality. We need continued and sustained investment to keep HIV prevention research on track to provide the additional tools that are required for sustainable, durable control of the HIV epidemic.”
The US government continued to be the major funder of HIV prevention research, contributing almost three-fourths of overall funding. A decrease of almost six percent, though, brought funding to a five-year low of US$830 million. The Working Group noted that sharp declines in US government funding have a major impact on the biomedical HIV prevention R&D field. With uncertainty around continued political will to fund the HIV response, this trend is extremely worrying.
Together, the US public sector and the Bill & Melinda Gates Foundation (BMGF) represented 87 percent of the total global investment in 2017, an imbalance that has continued for several years. The Working Group in this year’s report cautioned against the disproportionate impact of shifting donor priorities by these two donors on cutting-edge research, noting that a US$50 million decrease in vaccine R&D in 2017 was largely attributed to cuts from the US government, while a 67 percent increase in VMMC funding in 2017 is due largely to enhanced investment from BMGF. The Working Group renewed a call to diversify the funding base to ensure both the sustainability of the field and that decades of gains made in scientific innovation are not lost to fluctuating investment.
The Working Group noted with concern that funding by the European Commission (EC) dropped by almost half from 2016 to 2017 (US$14.4 million in 2016 to US$7.6 million). Noting increases in public sector funding from Canada, Brazil and the Netherlands, the Working Group called on other European countries to increase investment in critical HIV prevention tools to help end the epidemic and to offset the drop in EC funding.
“A true end to AIDS will only be possible if we can develop and deploy an effective, accessible HIV vaccine and other biomedical innovations to prevent HIV infection,” said Mark Feinberg, M.D., Ph.D., President and CEO of the International AIDS Vaccine Initiative. “Decades of research are paying off with the most exciting advances we’ve seen to date. But progress can only continue with sustained public and private sector investment in HIV prevention R&D.”
As researchers, implementers, advocates and funders gather this week in Madrid to review progress in HIV prevention research, there is much to be optimistic about in HIV science and in the accumulated knowledge of how to end the epidemic. At the same time, sobering changes in the funding and policy environment could imperil future progress and wipe out the progress made. Funding constraints, policy changes, shifting donor priorities and shifting demographics will all play a role in the world’s ability to respond to the continued challenges that HIV presents.
“With 5000 people becoming infected with HIV every day it is critical that we both scale up the effective HIV prevention programmes we currently have and invest in new technologies and solutions so that they can become a reality for the populations most affected by HIV,” said Tim Martineau, Deputy Executive Director, Programme a.i. UNAIDS. “Doing both will avert new infections, save lives and reduce the rising costs of life-long antiretroviral treatment.”
The report and infographics on prevention research investment are online at www.hivresourcetracking.org and on social media with #HIVPxinvestment.
###
Since 2000, the Resource Tracking for HIV Prevention R&D Working Group (formerly the HIV Vaccines & Microbicides Resource Tracking Working Group) has employed a comprehensive methodology to track trends in research and development (R&D) investments and expenditures for biomedical HIV prevention options. AVAC leads the secretariat of the Working Group, that also includes the International AIDS Vaccine Initiative (IAVI) and the Joint United Nations Programme on HIV/AIDS (UNAIDS). This year’s report is additionally made possible by the support of several donors, including the Bill & Melinda Gates Foundation and the American people through the US President’s Emergency Plan for AIDS Relief (PEPFAR) and the US Agency for International Development (USAID). The contents are the responsibility of AVAC and the Working Group and do not necessarily reflect the views of PEPFAR, USAID or the United States Government. AVAC does not accept funding from the pharmaceutical industry.
No Prevention, No End – AVAC launches new report and call to action
Today AVAC released No Prevention, No End, our 2018 annual report on the state of the field. Starting from the title—which humbly borrows the cadence of the call for an end to state-sanctioned violence against Black Americans, “No Justice, No Peace”—through to the closing words, “This is the worst possible moment for slowing down,” the Report is a call to action and guide for addressing the HIV prevention crisis that threatens progress in curtailing epidemics worldwide.
Click here to download the Report and individual sections and graphics; click here for a new episode of the Px Pulse podcast which covers the Report’s key themes and features lead author Emily Bass, AVAC’s Director of Strategy and Content.
UNAIDS named the prevention crisis in its July 2018 report, Miles to Go. It acknowledged that the scale-up of antiretroviral treatment, while essential, is insufficient as a prevention strategy. AVAC has been warning of an imbalance in approaches and investments across approaches, and calling for ambitious targets matched with political will, financing, timelines and more since the UNAIDS targets were first launched in 2014. (Check out AVAC Report 2014/5: Prevention on the Line for a summary of this critique of targets.)
In this year’s Report, we call out three core problems with primary prevention and the global HIV response, identifying the risks they bring and the path to a solution. Specifically, we focus on:
- Investing in demand creation: The private-sector gloss on this term cannot obscure its essential role in making primary prevention work. Strategies that might save lives are condemned as unwanted or unfeasible when they’re delivered in programs that lack integrated demand-side thinking, which is a science and not a set of slogans.
- Making informed choice central to HIV prevention: Programs that offer more than one option, along with a supportive environment for a provider and client to discuss risks, benefits and personal preferences aren’t a luxury but a necessity. The family planning field has metrics to measure choice; HIV should pick these up, with prevention programs leading the way.
- Unstinting radical action: Progress in the global AIDS response is tenuous; so is the state of democratic institutions and the future of the planet. These interconnected issues require more bold action, including from countries that are aid beneficiaries, and from the citizens of those countries who unite to hold truth to power. In the HIV prevention context, this means accountability for primary prevention at every level, including research for next-generation options.
AVAC is launching this Report as many stakeholders in HIV prevention research gather in Madrid for the HIV Research for Prevention (R4P) conference. Visit our special R4P page to find us on-site and follow along from afar, to see how the themes of this year’s Report resonate in a global and wide-ranging discussion of HIV prevention research and implementation at a critical time.
May Episode of Px Pulse Podcast: HIV vaccine science, research, updates and advocacy
Check out the newest episode of Px Pulse on iTunes or at www.avac.org/px-pulse!
With HIV Vaccine Awareness Day (HVAD) in the spotlight earlier this month, AVAC’s May episode of Px Pulse features four experts steeped in HIV vaccine research. Together they help set expectations for where the field is now and where it is going.
Dr. Larry Corey, who leads the HIV Vaccine Trials Network (HVTN), explains how the AMP studies, HVTN 702 and HVTN 705 will each, in different ways, advance what the field knows about how to develop a vaccine for HIV.
Then, IAVI’s Dr. Kundai Chinyenze talks about efforts to ready for possible success, so that new tools work in the real world as well as they do in a clinical trial.
And two deeply experienced advocates, Bill Snow and Matthew Rose, talk about engaging with the science and preparing for research results.
For the full podcast, highlights and resources (including AVAC’s newest HIV Vaccine Awareness Day toolkit), visit here. Subscribe on iTunes to catch every episode!
HIV Vaccine Science, Research, Updates and Advocacy
With HIV Vaccine Awareness Day (HVAD) in the spotlight earlier this month, AVAC’s May episode of PxPulse features four experts steeped in HIV vaccine research. Together they help set expectations for where the field is now and where it is going.
HIV Vaccine Awareness Day 2018: Tools & more
HIV Vaccine Awareness Day, May 18, commemorates the vital and ongoing work to develop a vaccine against HIV. This work advances because of the ingenuity, courage and commitment of trial participants, host communities, funders, scientists and advocates. AVAC salutes the collective trust and sustained dedication to end the epidemic.
2018 is marked by great advances in research and important opportunities for advocacy. In addition to a host of tools AVAC updates annually to keep you current on this front, The Rise of Broadly Neutralizing Antibodies by AVAC founder and former Global HIV Vaccine Enterprise executive director Bill Snow offers a comprehensive look at antibody mediated prevention and its connection to vaccine research.
In case you missed it, check out the recording and slides from the May 17 webinar featuring Dr. Sandhya Vasan’s discussion on the legacy of RV144 and vaccine advocate Mark Hubbard’s take on today’s agenda for HIV vaccine advocacy.
The complete set of AVAC’s HVAD resources includes:
- A special advocacy publication, The Story Is…, looking at three major efficacy trials in the context of funding, advocacy, stakeholder engagement and primary prevention
- A package of infographics on key issues
- HIV Vaccines: Introductory Fact Sheet
- A PowerPoint presentation: HIV Vaccine Basics
- A selection of key messages related to HIV vaccine advocacy
And add to the conversation on social media at #HIVvaccineAware and #HVAD2018.
The Rise of Broadly Neutralizing Antibodies
Bill Snow founded AVAC and is the former Global HIV Vaccine Enterprise Executive Director.
Research on broadly neutralizing antibodies (bNAbs) is taking the field of HIV prevention science in new directions, with implications for new prevention interventions and vaccine development. There’s much to know and much to learn about these powerful instruments of the immune system.
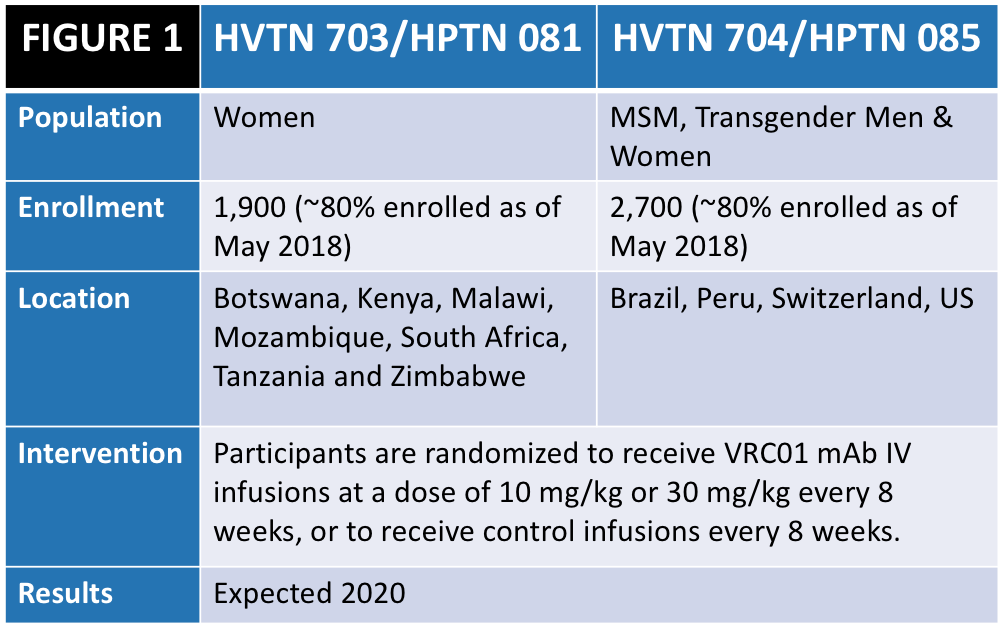
Since 2016, more than 2,700 men in Brazil, Peru, Switzerland and the US, and 1,900 women in Southern Africa have begun to enroll in clinical trials looking at antibody-mediated prevention, or AMP (see Figure 1). A collaboration between the HIV Prevention Trials Network (HPTN) and HIV Vaccine Trials Network (HVTN) (both funded by the National Institutes of Health), the AMP studies test the safety and efficacy of the broadly neutralizing antibody (bNAb) VRC01 when it is given every 8 weeks to reduce the risk of HIV infection. But how did this approach come about, why is it important and what may happen next with bNAbs for HIV prevention?
What’s an antibody?
Antibodies are Y-shaped proteins produced by B cells to clear infected cells and pathogens in the bloodstream. B cells are part of what is known as the adaptive immune system, which mounts defenses aimed at specific invaders—like a cold virus or chicken pox or HIV. The innate immune system also defends against invaders, but its defenses are not so finely tailored to a specific pathogen. When a virus encounters the right B cell, the B cell begins cloning itself and produces antibodies designed to battle that virus. These antibodies circulate throughout the body looking for the virus, and they evolve continuously, becoming ever more precise and numerous.
The Antibody Hierarchy
Here are some terms that will help you follow this ongoing story:
- Antibody: Proteins produced by B cells as a major part of the adaptive human immune defense against specific invaders.
- Binding antibody: An antibody that attaches to a virus but doesn’t necessarily render it ineffective; can be driven by the innate immune system.
- Monoclonal antibody: A bioengineered antibody made in a manufacturing facility by copying (cloning) one original antibody—selected for its potency and other characteristics.
- Neutralizing antibody: Antibody that disables virus.
- Broadly neutralizing antibody: An antibody that neutralizes many different genetic variants of HIV.
- Passive antibodies: A dose of monoclonal antibodies that are infused or injected, rather than made by one’s own immune system.