Today marks one year since AVAC and the Journalism Development Network worked with the Public Citizen Litigation Group to sue the US President, the State Department, the US Agency for International Development (USAID), and others, seeking emergency relief from a sweeping freeze on foreign assistance issued by the incoming administration that abruptly halted life-saving global health and development programs. A parallel case was brought by Global Health Council and partners and assigned to the same District Court judge, underscoring the broad concern across the global health community.
Twelve months later, these cases have come to symbolize a much larger question: whether the executive branch can override Congress’s constitutional authority over federal spending and dismantle decades of bipartisan foreign policy with the stroke of a pen, and whether the courts and Congress will fulfill their responsibilities to serve as checks on unbridled executive power.
The past year has laid bare the real-world consequences of unchecked executive action, threatening lives, destabilizing global partnerships, and undermining the United States’ credibility as a reliable partner.
An early ruling in AVAC’s case successfully unlocked nearly $2 billion in US government payments for work already completed, affirming that the executive branch cannot refuse to spend money appropriated by Congress. But over the course of 2025, appeals by the administration, ultimately backed by the US Supreme Court, ran down the clock on $4 billion in already-appropriated funds for the 2025 fiscal year, allowing them to expire.
While the Supreme Court’s ruling did not resolve the underlying constitutional questions, the decision was narrow and the Court left open the opportunity for further argument on the merit of the questions involved. In November 2025, a joint statement to the District Court requested to pause the cases, awaiting the outcome of other relevant court decisions.
The AVAC and GHC cases remain active, but lawsuits alone cannot restore what was lost—or undo the long-term harm caused by the sudden dismantling of global health systems.
The actions by this administration demand more than concern. This moment demands public accountability, sustained Congressional oversight, and durable legislative safeguards. Global health and equity require champions willing to fight for lives and livelihoods, and for what’s right. We cannot accept this as the new normal, and we must insist that Congressional authority, democratic governance, and the lives they protect still matter.
Global Health Watch: Reflecting on 1 Year of Chaos and What’s Next, Congress Pushes Back, the Future of WHO, US Undermines African Authority
Issue 52
This week marks 365 days of disruption and chaos across global health, with many organizations and journalists reflecting on one year after the foreign aid freeze and what the future of global health looks like. This week also saw the US Congress beginning to reassert its role on health funding, ongoing US disengagement from WHO, and new reporting on the hepatitis B vaccine trial in Guinea-Bissau.
We are also watching closely for news of an expanded Global Gag Rule, that is reportedly coming out later today, just as this issue goes to press. It is anticipated that this new gag will include a dramatic expansion beyond abortion and now underscore the US administration’s war on gender, diversity, equity and inclusion. We’ll cover this in next week’s Global Health Watch; the struggle, most definitely, continues.
365 Days of Chaos and Disruption, What Comes Next for Global Health
This week marks one year since the US Presidential administration issued a deeply cruel executive order freezing foreign assistance, halting billions of dollars in already-approved funding under the bad-faith claim of a “90-day review”. What followed was not a brief pause, but a drawn-out, chaotic disruption that stopped life-saving work across the globe, shutting down valuable organizations, and harming lives, health, and livelihoods. And that was just the beginning of a year of chaos. Many organizations and media coverage noted a growing recognition that the past year’s disruptions to global health were not just destructive, but catalytic, forcing a reckoning with how systems are built and for whom. Reporting from Bhekisisa reflected on how the sudden halt in US HIV funding exposed deep vulnerabilities in over-reliance on external aid, while also accelerating conversations about domestic financing, integration, and sustainability in the HIV response moving into 2026. At the same time, analyses fromHealth Policy Watch, Science, Nature, and The Lancet laid bare the human and scientific costs of abrupt policy shifts, shuttered programs, fractured research networks, and lost trust, while underscoring that simply restoring old funding streams will not be enough to meet future challenges.
IMPLICATIONS: Together, these stories and analyses point to the need to rethink and rebuild with stronger country ownership, diversified and predictable financing, resilient research institutions, and governance structures that prioritize equity, accountability, and community leadership. Rather than recreating the same architecture, reimagined global health systems must be less dependent on external donors and political ideology. As Global Health Watch has tracked for 52 weeks, the path forward is not about returning to the pre-foreign aid freeze status quo, but about using this period of disruption to construct a more durable, equitable, and responsive global health architecture. As Canadian Prime Minister, Mark Carney, said so clearly at this week’s World Economic Forum in Davos, Switzerland, “Nostalgia is not a strategy.”
Congress Steps Up In Defending Domestic and Global Health
The US Congress is beginning to reassert its constitutional role in shaping federal spending. The joint House and Senate FY26 funding bill released last week covering foreign operations would maintain funding for core global health priorities, including HIV, tuberculosis, malaria, polio, family planning and reproductive health, neglected tropical diseases, Gavi, and UN agencies such as UNAIDS, UNICEF, and UNFPA. This week, legislators rejected nearly $2 billion in proposed cuts to US domestic HIV and related programs through the Labor, Health and Human Services Education and Related Appropriations Act (LHHS), a “major victory” credited to sustained advocacy by people living with HIV, advocates, and service providers. The proposed bill largely preserves funding for domestic public health and biomedical research. As AVAC’s Suraj Madoori said in a statement, “These crucial wins for global and domestic HIV now require us to not hold back, and urge Congress to swiftly approve all the FY26 bills, push the President to sign them, and for us to ensure accountability in the administration to spend and implement this lifesaving funding as instructed by the people and those who represent us in Washington D.C.”
IMPLICATIONS: Together, these bills signal a return to a bipartisan appropriations process and, if enacted, provide a basis to push back against unilateral cuts by the administration. They also signal bipartisan pushback against attempts to cut health and scientific research investments. By rejecting the steep cuts proposed by the administration, they stabilize lifesaving programs and protect the research enterprise. The House passed the bills on Thursday, and the focus now shifts to the Senate, which must pass the bills by January 30. Then onto the President to sign, and, most critically, for the administration to actually spend all Congressionally appropriated funds.
This week also marks one year since the US announced its intended departure from World Health Organization (WHO). Debate over its future and the US’ role within it intensified as pressure from parts of the administration collided with growing concern over the consequences of disengagement. US officials and policymakers aligned with the “America First” strategy call for WHO to be fundamentally reformed or replaced. Analysts note that the US remains a formal member of WHO until debts are paid. Meanwhile, the US administration continues to withhold funding and delay payments, leaving millions of dollars in unpaid US obligations.
IMPLICATIONS: The current state, where the US remains technically engaged but substantively absent, poses serious risks for global health governance, disease surveillance and pandemic preparedness. As analyses from CSIS underscores, WHO reform is both necessary and possible, but meaningful reform requires constructive engagement, predictable financing, and political leadership, not abandonment.
Hepatitis B Vaccine Trial in Guinea-Bissau Undermines African Authority
Reporting this week is exposing a pattern of US actions that show deep disregard for African public health leadership, ethical research standards, and sovereignty. The US-funded hepatitis B vaccine trial in Guinea-Bissau is at the center of this. As we reported in previous weeks, the unethical trial would delay birth-dose vaccination for thousands of newborns despite overwhelming evidence, and WHO guidance, that immediate vaccination saves lives. According to Rolling Stone, the study was championed by US officials aligned with anti-vaccine ideology and advanced even as Africa CDC officials raised alarm and indicated the trial should be halted. At the same time, the US administration has been marginalizing Africa CDC more broadly, cutting engagement, undermining its authority, and sidelining African institutions in favor of unilateral decision-making. This is being reinforced, as The Guardian reports, by members of the US administration urging US diplomats to emphasize American “generosity” to African leaders even as USAID programs are shuttered and health funding withdrawn.
IMPLICATIONS: Together, these developments signal a dangerous erosion of respect for African expertise, autonomy, and ethical authority in global health. Pushing forward research designs that would withhold proven interventions—while dismissing objections from Africa CDC and African scientists—revives patterns of extractive and unethical research long condemned by the global health community. Undermining Africa CDC while advancing ethically dubious trials weakens trust, damages partnerships, and threatens progress against hepatitis B, HIV, and other diseases where Africa has led with scientific excellence.
This five-part series reflects on the tumultuous events of the past 365 days across five global health issues: the erosion of US foreign aid; dismantling of the research enterprise; attacks on vaccine policy; and shifts in the global health architecture.
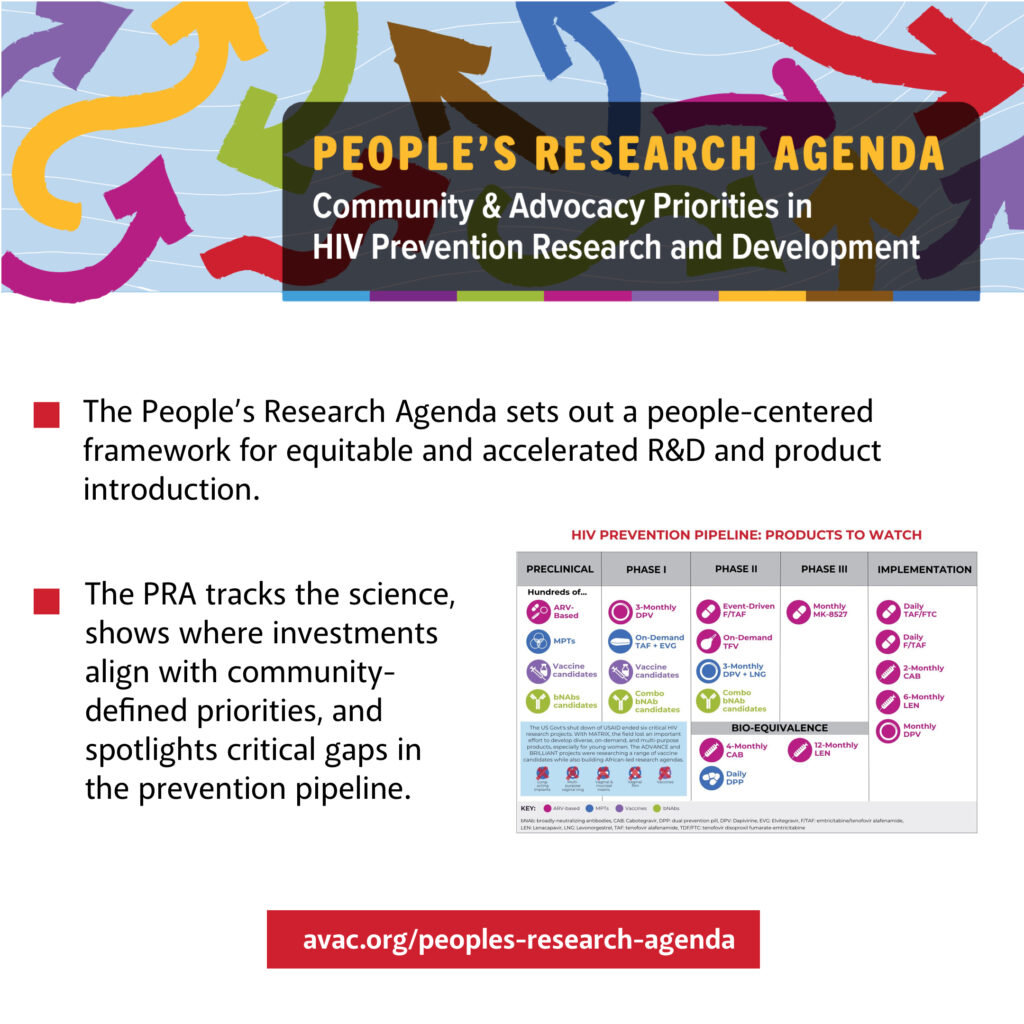
As new IDSA CEO, Jeanne Marrazzo warned in a webinar this week, rising HIV infections threaten progress, but “this is not a time to despair. It’s a time to fight.” Watch the recording and explore the 2025 People’s Research Agenda, which tracks the science, flags gaps, and centers community priorities to keep HIV prevention moving forward.
Our Reflections on Foreign Aid, Vaccine Science, Research Opportunities and the Future of Global Health
“The last year has been one of chaos, anger, panic, and frustration. I think the coming year has to be one of strategic rebuilding and building something different—not building back but building forward. That means a different architecture at the country level, community level, regional level, and global level. A year from now, I suspect we’ll see fewer acronyms, but hopefully the ones that remain will be stronger than ever.” —AVAC’s Mitchell Warren, Bhekisisa podcast
This week marks one year since the US Presidential Administration issued a deeply cruel executive order freezing foreign assistance, halting billions of dollars in already-approved funding under the bad-faith claim of a “90-day review”. What followed was not a brief pause, but a drawn-out, chaotic disruption that stopped life-saving work across the globe, shutting down valuable organizations, and harming lives, health, and livelihoods. And that was just the beginning of a year of chaos.
To mark this moment, AVAC’s One Year Later series reflects on the impact of the past 365 days on five key areas of global health and development:
These pieces show how the field navigated a year defined by disruption and resilience—and how policy decisions reverberate through science, programs, and communities.
The year has been a profoundly transformative one for AVAC. The Devex in-depth retrospective, Fighting for Billions: The legal battle to keep US foreign aid alive, chronicles the ongoing lawsuits brought by AVAC, the Global Health Council and partners challenging the foreign aid freeze. The piece highlights how legal action became a critical line of defense against the dismantling of lifesaving programs and why the outcome still matters.
“For me, the best message I can say is a year later, we as a community are still standing. And that is a resilience in its own right. We are going to succeed in global health and development. Not because of what happened in the last year, but in spite of it.”
—AVAC’s executive director Mitchell Warren on Bhekisisa’s new podcast, One year after Trump: The day HIV funding changed forever—and what came next
As Jeanne Marrazzo, the new CEO of the Infectious Diseases Society of America (IDSA) shared on our webinar earlier this week showcasing the 2025 update of the People’s Research Agenda (PRA), “We cannot yell it from the rooftops loud enough that new infections are going to rise and undermine efforts to end AIDS as a public health threat. But this is not a time to despair. It’s a time to fight. It’s a time to dig in and recognize not just what we’ve accomplished and why we need to protect that, but why we need to continue to move forward.” See the recording here and learn more about the PRA, which tracks the science, highlights where investments align—or fail to align—with community priorities and identifies critical gaps that must be addressed to ensure the prevention pipeline meets the needs of diverse populations.
The past year has reshaped global health—and AVAC—in ways that will be felt for years to come. The events of the past year also show that advocacy, evidence, and community leadership matter. Some courts provided the necessary check on power; advocates rallied; and scientists and civil society raised their voices and documented what was lost—and what must be protected (see 24 Hours to Save AIDS Research).
With your support, AVAC’s weekly Global Health Watch newsletter, now in its 52nd week, continues to track what happens, elevate what’s at risk, and help all of us navigate what comes next. Thank you to our community which stops at nothing to safeguard hard-won progress against HIV and in advancing global health equity.
Global Health Watch: A Year That Reshaped Global Health
The Lancet journal ended the year with a provocative editorial – 2025: an annus horribilis for health in the USA. But sadly, it was not just in the US; it has been a year of chaos and disruption globally. This 49th issue of Global Health Watch looks back—like many news stories this week—across 2025 to highlight the most consequential decisions, disruptions, and debates that defined the year and will continue to shape what comes next.
The Foreign Aid Freeze and the Legal Fight to Restore it
On the first day in office, the new US Administration issued a sweeping foreign aid freeze that halted life-saving global health and HIV programs, severed active grants, research underway and cost millions of people their lives and livelihoods. In less than a month, AVAC responded suing the President, the State Department and the US Agency for International Development (USAID). The Global Health Council also led a similar lawsuit challenging the freeze as unlawful and harmful. Together, the two cases argued for months in various courts that the foreign aid freeze not only jeopardized health as a human right but also bypassed congressional authority and undermined trust in US leadership. Ultimately, the cases unlocked millions of dollars of development assistance for work done in January and February, but millions more dollars expired at the end of the fiscal year in September. The cases are ongoing and as important as ever, both to restore foreign assistance and to re-assert that it is Congress (and not the President) who has the power of the purse.
Science faced underfunding and systematic destabilization in 2025. In just one month under the new US Administration, the National Institutes of Health (NIH) abruptly canceled approximately 1,800 research grants. By April, mass layoffs and forced reassignments across Health and Human Services (HHS) agencies, including the Centers for Disease Control and Prevention (CDC), NIH, and US Food and Drug Administration (FDA), further crippled each agency’s capacity and expertise. A proposal to drastically cut the overall NIH budget and consolidate its 27 institutes was soon introduced along with the fiscal year 2026 budget, which proposed an $18 billion cut from the NIH and $1.5B cut in HIV prevention. Around the same time, the NIH signaled a major shift away from investments in basic science and clinical research, undermining the discovery pipeline that fuels future breakthroughs. Then, in November, HHS ordered the CDC to phase out all “non-essential” nonhuman primate research, threatening foundational preclinical studies, including those that have been pivotal to HIV PrEP and PEP, amongst many other health priorities. These actions were compounded by a pause or effective ban on some international research collaborations, a proposed cap on indirect cost rates that support core university infrastructure, and changes to the scientific review processes, together weakening the systems that sustain rigorous, independent research.
The Cruel Irony of the Best Shot at HIV Prevention
Despite all the chaos, 2025 offered remarkable milestones in HIV prevention science, and a stark illustration of the contradictions shaping global health. Injectable lenacapavir for PrEP (LEN), the six-month injectable, which provides nearly complete protection against HIV infection, moved with unprecedented speed from regulatory approvals and guidelines to real-world introduction. South Africa and Zambia authorized LEN within months of US and EU regulatory approvals; the World Health Organization (WHO) rapidly issued guidance and prequalification; and initial LEN delivery began in Brazil, Eswatini, South Africa, and Zambia, setting the stage for expanded access in 2026. At the same time, efficacy trials began of the next promising PrEP option, the monthly oral candidate MK-8527, reinforcing what’s possible when innovation, evidence, and advocacy align.
Yet, all this scientific momentum occurred alongside the deepest assault on global health and the systems that make it possible. The cruel irony of this moment is that as the science breaks barriers, the infrastructure meant to support discovery, evaluation, and equitable delivery is being weakened, threatening the very gains the field has fought decades to achieve. As AVAC has emphasized, the greatest opportunity in HIV prevention lies in speed, scale, and equity.
Actions in the last 11 months have eroded evidence-based policy, disrupted institutional capacities, and deepened mistrust and uncertainty in vaccine science. In May, NIH’s National Institute of Allergy and Infectious Diseases (NIAID) announced that funding for the Consortia for HIV/AIDS Vaccine Development (CHAVD) would end after the current grant cycle in June 2026 — eliminating $67 million annually and about 10% of global HIV vaccine research funding. Then, $500 million in Biomedical Advanced Research Development Authority (BARDA) grants for research and development of the mRNA vaccine platform were soon cancelled, and members of the CDC’s Advisory Committee on Immunization Practices (ACIP) were replaced. The US also stopped supporting Gavi, the vaccine alliance, and language on the CDC website was replaced with anti-science and anti-vaccine sentiment. As AVAC said in an August statement, “These actions dangerously sow vaccine disinformation and mistrust, which has proliferated since the COVID-19 pandemic. Dangerous ideology results in dangerous policymaking, putting many lives at stake and complicating efforts to both discover and implement clinical and cost-effective interventions to make America and the world healthier, safer, and more prosperous.”
As rising nationalism, geopolitical tensions, and funding retrenchment intensify, the architecture of global health and how countries engage in it and with one another is being fundamentally reshaped. Longstanding multilateral systems are giving way to a more fragmented, country-to-country model under the US America First Global Health Strategy. The strategy prioritizes bilateral health Memorandums of Understanding (MoUs) with individual countries in exchange for funding support, data sharing, and pathogen access, signaling a major recalibration away from traditional multilateral institutions and frameworks. Meanwhile, the US stepped back from longstanding global health platforms including an unprecedented absence at the World Health Assembly, withdrawal from the WHO, and diminishing support for joint initiatives like Gavi, the vaccine alliance. Civil society and advocates are actively debating what this means for shared goals and equity in global health, even as institutions like WHO and UNAIDS explore how to adapt in a rapidly evolving landscape.
Global Health Watch: UNAIDS launches review, NIH GoF controversy, support for IDSA’s Jeanne Marrazzo, UK authorizes LEN for PrEP
This week the UNAIDS board approved a new Global AIDS Strategy and launched a formal review of the agency’s future; turmoil at the NIH continues over gain-of-function research; and the scientific community rallies around the Infectious Diseases Society of America’s (IDSA) appointment of Jeanne Marrazzo as its chief executive officer. Also, the UK regulatory agency approved lenacapavir for PrEP (LEN) marking its seventh regulatory approval in just six months.
UNAIDS Launches Review Process on its Future
Following last week’s intense discussions at the UNAIDS Programme Coordinating Board (PCB), the UNAIDS board this week launched a new, formal process to examine the organization’s future and potential transition pathways. This comes from within the UN80 reform initiative that proposed to sunset UNAIDS by the end of 2026. But civil society and PCB members pushed back, and the board agreed to initiate a “structured review” that explores different scenarios for UNAIDS’ role, mandate, and positioning within a changing global health architecture. This announcement came on the heels of the PCB approving the Global AIDS Strategy for 2026–2031 and alarms raised by civil society about funding cuts, service disruptions, and the risk of losing a central coordinating body at a critical moment in the HIV response.
IMPLICATIONS: The launch of this process to examine UNAIDS’ future raises important questions about governance, accountability, and continuity in the global HIV response. Civil society’s strong pushback underscores that any reform must preserve UNAIDS’ core mandate and ensure that the global HIV response remains centered on those most affected — especially women, girls, and key populations — rather than being quietly dismantled at a moment of crisis.
Continued Turmoil at the NIH – Gain-of-Function (GOF) Research
Turmoil at the NIH continued this week as, John Beigel, a prominent influenza researcher and acting director of NIAID’s Division of Microbiology and Infectious Diseases (DMID), resigned following controversy over an NIH-supported seasonal flu virus study and how its potential risks were assessed and communicated. Beigel’s departure unfolds amid ongoing debate over how the NIH defines and oversees gain-of-function (GOF) research—work that could increase the transmissibility or virulence of pathogens with pandemic potential.
Science reports that the controversy was a “‘pseudomanufactured concern’ that was meant to force him out, so officials could bring in a researcher who has strongly supported Trump.” Beigel is being replaced by an infectious disease scientist from NIH’s Fogarty International Center and who has publicly expressed support for the President and donated to his affiliated political committees.
IMPLICATIONS: Alongside last week’s revelations and Jeanne Marrazzo’s whistleblower lawsuit, Beigel’s departure heightens concerns about instability and governance at NIH at a time when scientific leadership and public trust are critical. Debates over GOF research, including its definition, oversight, and whether the White House or the NIH sets the rules show the precariousness of the agency. As Science reports, concerns about GOF work have gained momentum with the popularization of the belief that Chinese scientists who received NIH funding created the virus that caused the COVID-19 pandemic. Many Republicans have promoted this unproven theory, and Trump signed an executive order in May that called for stricter oversight of GOF work.
Leaders Support Jeanne Marrazzo as new CEO of the Infectious Diseases Society of America (IDSA)
Leaders in the scientific and infectious disease communities praised the Infectious Diseases Society of America (IDSA) appointment of Jeanne Marrazzo as its next chief executive officer. Former NIAID Director Anthony Fauci called her a “superb choice,” and AVAC’s Mitchell Warren said, “It speaks to IDSA’s desire to emphasize science over politics and science over ideology, and that’s what you will get with Jeanne Marrazzo.” Virologist Angela Rasmussen, said Marrazzo’s appointment “suggests to everybody who’s a member of that professional society that they’ve got a leader who’s actually going to do something about this rather than trying to protect the institution more than its members.” Marrazzo begins her tenure January 12.
UK’s Medicines and Healthcare products Regulatory Agency (MHRA) Approves LEN for PrEP
This is the seventh regulatory approval of LEN for PrEP. See AVAC’s detailed map of regulatory approvals, pending decisions, and appeals, along with other LEN resources here.
This month, AVAC marked our 30th anniversary. Over three decades, the HIV field has evolved dramatically—but what we do, and why we do it, has remained constant: standing for science, equity, and community leadership, and ensuring evidence drives decisions that affect people’s lives. We’ve been able to do this work because of your partnership and support, and we are deeply grateful.
Last week, we also released the 2025 update of the People’s Research Agenda (PRA), which tracks the science, highlights where investments align—or fail to align—with community priorities, and identifies critical gaps that must be addressed to ensure the prevention pipeline meets the needs of diverse populations. After ten months of disruption and uncertainty across biomedical research and global health, we hope this agenda helps share a path forward, one that will demand sharper priorities, smarter investments, and a balanced portfolio focused on real epidemic impact.
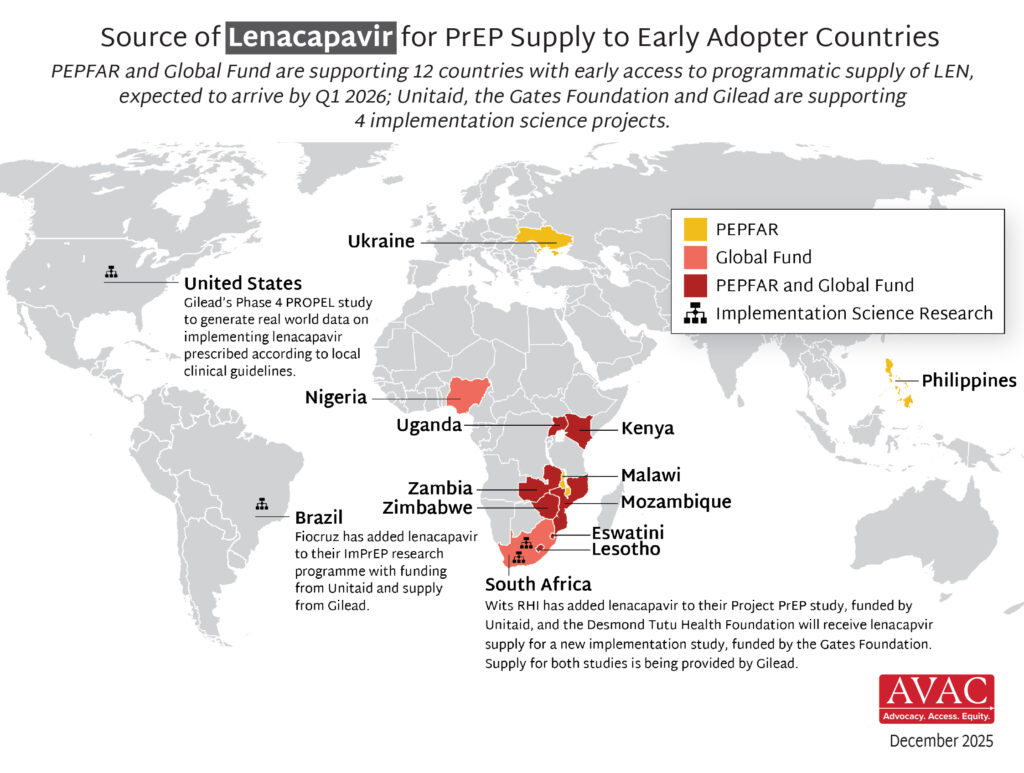
At the same time, we are seeing real progress. In just the past month, people in Brazil, Eswatini, South Africa, and Zambia began receiving the first doses of lenacapavir for PrEP (LEN) through early implementation programs outside the US, with additional deliveries of LEN planned for Eswatini, Zambia, Kenya, Lesotho, Mozambique, Nigeria, Uganda, and Zimbabwe.
As we enter our fourth decade, your support makes it possible for AVAC to keep tracking the science, elevating community priorities, and delivering real-time analysis when it matters most. If you’re able, we invite you to consider making a year-end gift to sustain this work.
Thank you for being part of this work, and for standing with AVAC.
Global Health Watch: NIH turmoil + a high-profile lawsuit, future of UNAIDS, more Countries sign “America First” MoUs with US
Issue 47
This week covers the significant turmoil at the US National Institutes of Health (NIH), including a close look at the NIH deputy director’s role in disruptions in leadership and funding cuts, and a lawsuit filed by the former Director of the National Institute of Allergy and Infectious Diseases (NIAID). It also covers urgent civil society pushback against efforts to sunset UNAIDS, the rapid expansion of US “America First” bilateral health agreements across Africa, and what’s next for STI research, prevention and diagnostics.
NIH Leadership Turmoil
A new investigation by The Atlantic’s Katherine Wu examines the central role of the Deputy Director of the National Institutes of Health (NIH), Matthew Memoli, in recent leadership changes and funding cuts across the NIH, including the firing of former NIAID Director, Jeanne Marrazzo, and the reassignment of Carl Dieffenbach, longtime director of NIAID’s Division of AIDS, to another NIH center. The Atlantic’s reporting shows how these decisions have significantly weakened NIAID, with particularly acute impacts on HIV prevention and vaccine research, where programs, expertise, and long-term scientific capacity are being eroded amid broader restructuring and budget shifts.
In addition, this week, Dr. Marrazzo, the newly appointed chief executive officer of the Infectious Diseases Society of America (IDSA), filed a lawsuit against the US federal government. The lawsuit alleges that Marrazzo was illegally fired from her position and seeks to be reinstated as head of NIAID and to receive formal declarations that her rights were violated. The suit argues that her firing was retaliation for a whistleblower complaint she filed on September 3, in which she raised concerns about anti-vaccine positions held by newly appointed NIH officials; demands to halt clinical trials; and requests to cut international research collaborations. Twenty-two days after filing the complaint, Marrazzo was fired by Health and Human Services Secretary, Robert F. Kennedy Jr.
IMPLICATIONS: The developments at the NIH show instability at its leadership level and severe consequences for infectious disease research, particularly vaccine research. This comes at a time when sustained R&D investment is most critical. Without robust research support, future advances in next-generation options could stall. See the new People’s Research Agenda, which calls for a balanced HIV prevention portfolio that is optimized for impact. However, Marrazzo’s new role at the IDSA, which represents clinicians, scientists and public health experts who are driving policy and advocacy to address critical issues in combating infectious disease, will be pivotal in ensuring rigorous science, inclusion and equity in research, community engagement, and evidence-based communications remain central to tenors in global health discourse and debate.
Member states and civil society convened at the 57th meeting of the UNAIDS Programme Coordinating Board (PCB) in Brazil this week to discuss urgent decisions about the future of the global HIV response amid deep funding cuts and a shifting global health landscape. They reviewed and approved the Global AIDS Strategy 2026–2031 and assessed the impact on communities from disruptions to services for HIV prevention and treatment. Civil society representatives on the PCB shared comments, and African women leaders and other civil society groups issued statements (and sign-ons) denouncing efforts to sunset UNAIDS by the end of 2026: “Any move to sunset UNAIDS before ending AIDS as a public health threat is premature and unacceptable. No sunsetting until we finish the job. AIDS is not over.”
The PCB also held a special thematic session on long-acting ARVs for treatment and prevention. See this clip from Yvette Raphael where she included AVAC’s latest blog in her remarks about the current context: “We cannot let cruel international policy allow historic gains to collapse, just as a few highly effective prevention options arrive. That is why rolling out LEN to all countries that need it with speed, scale and equity must be our uncompromised, uncompromising priority. If we do this, we can change the trajectory of the epidemic, but only if we act at the pace that data and science demand.”
IMPLICATIONS: As the world moves toward the June 2026 High-Level Meeting on HIV, and the rollout of the new Global AIDS Strategy, the strong pushback by civil society at the PCB underscores that any reform must preserve UNAIDS’ core mandate and ensure that the global HIV response remains centered on those most affected — especially women, girls, and key populations — rather than being quietly dismantled at a moment of crisis.
Eswatini and Mozambique Join Growing List of African Countries to Sign “America First” Bilateral Health MoUs
Mozambique and Eswatini are the latest countries to sign the bilateral health Memorandums of Understanding (MoUs) with the United States under the America First Global Health Strategy, adding to earlier agreements with Kenya, Liberia, Rwanda and Uganda. These agreements provide 5 to 10 years of funding and health support in exchange for co-financing, health data, pathogen-specimens, and national health system data, marking a major shift in how global health cooperation is structured under US leadership.
IMPLICATIONS: The pace of these agreements shows how quickly the Administration is moving to reshape US global health with little time for discussion and debate on transparency, consultation, and how civil society fits within this evolving framework. As the landscape shifts, civil society and non-governmental organizations must quickly reassess their roles in the hope of preserving aid delivery, accountability, and equity.
The Future of HIV Prevention Depends on Speed, Scale and Equity
“Every funding cut can represent at minimum, a delay. Every delay in rollout is a missed chance to prevent infections. Every un- or underfunded clinic is a barrier to access. Every policy is a choice to be inclusive or leave someone behind…”
AVAC’s STI program looks back at 2025—and ahead to 2026—tracking rising STI rates, major HPV vaccination gains, slow but promising diagnostics, the growing role of self-care, and what’s next for STI research, prevention and diagnostics.
AVAC Board Member Jeanne Marrazzo named CEO of IDSA
New York, NY, December 18, 2025 — AVAC enthusiastically applauds the selection of Jeanne Marrazzo, MD, to serve as the new chief executive officer of the Infectious Diseases Society of America (IDSA). Marrazzo brings outstanding leadership and research expertise to this role. She has demonstrated decades of unwavering commitment to research and advocacy for HIV and STI prevention, and a deep understanding of the importance of equity, accountability and trust in science, research and global health.
“Jeanne Marrazzo is an extraordinary choice and perfectly suited to lead IDSA and the larger infectious disease field into the future, especially at this particularly perilous moment,” said AVAC’s executive director, Mitchell Warren. “Her deep commitment to rigorous science, inclusion and equity in research, community engagement, and accurate, evidence-based communications is unparalleled — and is needed now more than ever.”
IDSA represents clinicians, scientists and public health experts from around the world, who are driving policy and advocacy to address critical issues in combating infectious disease, from workforce development to clinical guidelines to pandemic preparedness. Marrazzo’s vision, abiding integrity and leadership at IDSA will be a boon for the field.
Marrazzo, an AVAC board member, previously served as the director of the NIH’s National Institute of Allergy and infectious Disease (NIAID). Marrazzo was put on administrative leave by the new US presidential administration earlier this year and was formally dismissed from her position in September. She has consistently displayed extraordinary commitment, courage and leadership in responding to attacks on the NIH and on science generally.
“Her actions are a model for all who believe equity and evidence are the bedrock of science, research and health. We proudly stand with Dr. Marrazzo, and we look forward to her leadership and partnership in sustaining progress against HIV and other infectious diseases and in helping re-build trust and confidence in science and public health,” said Warren.
###
About AVAC AVAC is an international non-profit organization that provides an independent voice and leverages global partnerships to accelerate ethical development and equitable delivery of effective HIV prevention options, as part of a comprehensive and integrated pathway to global health equity. Follow AVAC on Bluesky and Instagram. Find more at www.avac.org and www.prepwatch.org.
Global Health Watch: PEPFAR negotiations leave communities behind, Global Fund replenishment falls short, continued chaos at CDC and NIH
Issue 44
UNAIDS World AIDS Day report: Overcoming disruption, transforming the AIDS response
Decisions and actions this week further weaken the global HIV response — from the exclusion of communities in the new PEPFAR US global health strategy negotiations to a Global Fund replenishment that falls short of what’s needed to deliver emerging HIV, TB, and malaria innovations at scale. Major disruptions at the US CDC and NIH – including halted non-human primate research, politicized vaccine messaging, leadership changes that jeopardize HIV research, and “skipping” World AIDS Day — continue the erosion of accountability, trust, and the integrity of the public health system.
US Global Health Strategy Negotiations Leaving Communities Behind
African advocacy partners including Eastern Africa National Networks of AIDS and Health Service Organizations (EANNASO) and the Coalition to build Momentum, Power, Activism, Strategy & Solidarity in Africa (COMPASS) have been taking stock of the ongoing country negotiations around the US government’s Memorandums of Understanding (MoUs) as part of its new “America First” global health strategy. They are finding that communities are being systematically excluded from the “government-to-government” negotiations for new 5-year PEPFAR MoUs, a direct reversal of the community engagement that has defined decades of the HIV response. Efforts to ensure program effectiveness, implementer accountability, programs for key populations, and commodity security are all at stake. The new framework would also require partner countries to share pathogens and patient data, potentially with US commercial interests, without privacy safeguards or assured access to resulting products — for decades longer than the life of the actual MOUs. With an MoU signing deadline of December 12, there is a great need to mobilize to demand transparency, inclusion and fair terms for all parties.
IMPLICATIONS: The exclusion of communities from the new MoU negotiations is an abrupt shift away from the community-centered model that has been at the center of PEPFAR’s success for decades. These closed-door, government-to-government negotiations undermine the hard-won progress on reaching key populations, protecting data privacy, and delivering services that are responsive to the real-life needs of communities. Sidelining communities threatens the effectiveness, and legitimacy of the next phase of the HIV response and without immediate transparency and meaningful engagement, these MoUs risk weakening impact and trust.
Global Fund Replenishment Support, But Falls Short of Target
Last Friday, donors pledged just over $11 billion at the Global Fund’s 8th Replenishment in Johannesburg. This was an important show of support, especially given the challenging political and economic climate, but well short of the $18 billion target needed to fully harness today’s unprecedented scientific advances against HIV, TB and malaria. The US pledged $4.6 billion, a decrease from the previous cycle, even as it reaffirms the 1:2 matching commitment, placing renewed pressure on Congress to fully appropriate funds, and on other donors to step up.
IMPLICATIONS: As long-acting HIV prevention, new malaria tools and improved TB treatments enter the market, this shortfall threatens the speed, scale and equity of their rollout. And with communities already facing service disruptions, this shortfall could cost millions of lives and squander a historic opportunity to turn innovation into impact.
Big Disruptions at US CDC and NIH – and World AIDS Day
In the last week, decisions and actions at the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health’s (NIH) Division of AIDS (DAIDS) further jeopardize the future of HIV research and confidence in vaccines. The CDC abruptly ordered an end to all non-human primate research, including critical macaque studies that have long supported HIV prevention science. The agency also altered language on its website implying a link to vaccines and autism and contradicting established scientific consensus. At the NIH, long-time DAIDS Director, Carl Dieffenbach, was reassigned to the Fogarty International Center, a move that removes a trusted leader who played a central role in guiding HIV research. See AVAC’s resource, HIV Prevention R&D at Risk, which tracks the impact of all this and more. Also, just ahead of December 1, the US administration announced that it will no longer commemorate World AIDS Day.
IMPLICATIONS: Together, these actions continue the decline in US global health leadership, unraveling decades of scientific progress and trust in vaccines and public health institutions. Halting essential preclinical research in macaques, politicizing vaccine messaging and sidelining experienced leadership weakens the pipeline of innovation and threatens the integrity of HIV science at a moment when sustained investment and credibility are most needed. As for World AIDS Day, Congressman Mark Pocan, who leads the Congressional HIV/AIDS Caucus, said the administration’s refusal was “shameful and dangerous.” But it’s important to remember that World AIDS Day is not decided by the US government; it belongs to everyone – and the new UNAIDS report provides the theme: Overcoming disruption, transforming the AIDS response. Or as the International AIDS Society says: Rethink. Rebuild. Rise.
UNAIDS World AIDS Day report: Overcoming disruption, transforming the AIDS response
UNAIDS’ new report shows that we were closer than in decades to ending AIDS by 2030, yet new HIV infections stayed flat in 2024, even before funding cuts, and resources were not enough to drive them down. We must double down with bolder, more strategic action to drive real decline.
Global Health Watch: Global Fund replenishment, LEN for PrEP arrives, HIV funding uncertain post gov’t shutdown
Issue 43
This week’s newsletter publishes just as the Global Fund’s 8th Replenishment Summit in South Africa is taking place. The Global Fund represents one of the strongest symbols of global solidarity in the fight against HIV, TB, and malaria, but, despite early pledges from several European Union member states and private partners, key donors (including the UK, Germany and France) appear to be stepping back, with smaller or uncertain pledges at this critical moment, and it is not yet clear what the US will do. A budget-constrained Global Fund raises serious concerns about losing ground against all three diseases and failing to seize opportunities to scale up new innovations in all three, including long-acting injectable PrEP for HIV. This Global Fund Advocates Network (GFAN) tracker tallies pledges, and this resource for scenario building shows how potential donor pledges could impact the funds available for health programs. Be sure to watch AVAC’s channels for the latest on the pledges.
Read on for more including the arrival of injectable lenacapavir for PrEP in Eswatini and Zambia, the uncertain future of US health funding post-shutdown, and new research exposing the impact of NIH clinical trial cuts.
Lenacapavir Arrives in Eswatini and Zambia
The first doses of injectable lenacapavir for PrEP (LEN) arrived in Eswatini and Zambia. These initial deliveries mark a historic acceleration in PrEP access, moving faster than we’ve seen with past introductions (see AVAC’s new graphic comparing the rollout of LEN to past PrEP products) and signaling momentum and an ability to apply lessons from past delays. With additional regulatory reviews underway across the region, this early action represents a promising step forward.
IMPLICATIONS: While these first shipments are worth celebrating, they’re just a down payment on what’s needed to deliver LEN at scale with equity. The joint Global Fund and PEPFAR commitment to reach two million people in the first three years is far more ambitious than past introductions, but falls short of delivering the impact that is needed. For LEN to have maximum impact, global donors and governments must align on transparent volume commitments, prioritize high-need markets and ensure that rollout strategies are rooted in community-led approaches. While South Africa is slated to receive LEN with Global Fund support, the fact that they are excluded from PEPFAR’s program is a huge, missed opportunity. If we really want to build a sustainable market as quickly as possible, one that will drive volume up and prices down and deliver real impact, South Africa must be THE center of the market and needs PEPFAR and Global Fund both to work with the South Africa government. AVAC’s full LEN resource library, including infographics on supply and demand, is designed to support advocates working to make that vision real.
US Government Reopens, Health Funding Remains Uncertain
The US Congress officially reopened the federal government after the longest shutdown (43 days) in the country’s history. Funding for most agencies is now extended until January 30, and three appropriations bills were passed to cover several departments through all of fiscal year 2026 which ends next September. However, key health initiatives remain vulnerable: the deal keeps major health programs, including the nation’s HIV response, on a short-term continuing resolution only through January, and does not address spiking US health insurance costs.
IMPLICATIONS: HIV prevention, treatment, and care programs will continue at last year’s levels through January 30, which avoid devastating cuts for the time being, with the fight to increase investments ongoing. The broader budget agreement also sidesteps major reforms demanded by lawmakers that threaten to gut these programs. It’s not clear if or when future disruptions might further impact public health programs and US global health engagement.
Clinical Trials Affected by NIH Research Grant Terminations
A new study published in the Journal of the American Medical Association (JAMA) shows that more than 74,000 clinical trial participants were affected when 383 clinical trials lost funding from the National Institutes of Health (NIH) between February 28 and August 15, 2025. These cuts disrupted research across a range of diseases, but most of the targeted trials were outside of the US and were testing preventive or behavioral interventions, primarily in infectious diseases. “Those findings suggest that there’s a bias towards termination of grants that have nothing to do with the quality of research being conducted,” the authors wrote.
IMPLICATIONS: This is one of the first studies to officially document the impact of the Presidential Administrations’ hostile policies and funding cuts to science. The political willingness to gut science without warning erodes trust in public health institutions and undercuts the foundation of long-term innovation. The impact is being seen across geographies, industries, communities, and diseases.