In the days, months and years ahead under a new US Presidential Administration, advocacy for choice, freedom, science, and rights will require intentional strategies to protect hard fought gains in HIV treatment and prevention and in global health generally, and to safeguard policies and programs that advance it. And there will be major implications for the global AIDS response.
Navigating through the work ahead involves assessing the potential impact on PEPFAR and Global Fund support; on USAID, NIH, CDC and the FDA; on the US relationship to WHO and other UN agencies; and on evidence- and rights-based policies and programs generally. Joining us to begin those efforts and better understand the landscape for advocacy are Jen Kates from KFF and our own Suraj Madoori.
This Week at AVAC: US election, new LEN resources, STI pipeline and PrEP service delivery
As we continue to grapple with the results of the US presidential election and what this means for our work and for global health evidence- and rights-based policies and programs generally, we wanted to share a range of new tools and resources you may find helpful in your advocacy for choice, science and rights.
Understanding Anal Pleasure and Health for Clinicians, Behavioral Health Specialists, Peers & HIV Workers
Forty years into the epidemic, people are still seeking accurate, reliable information about anal play that isn’t just about HIV and STI prevention. They want to understand how to engage in ways that maximize pleasure and reduce harms beyond infectious disease. Often, they end up encountering harmful myths rather than facts, and then learn by ‘trial and error’.
This 90-minute webinar is appropriate for HIV and STI clinicians, behavioral health workers, social workers, case managers, peers and anyone else with a responsibility for delivering or referring to HIV services like treatment, PrEP, testing and support services.
Participants learned the rationale for why addressing anal pleasure and health is essential in HIV service settings as well as ways to respond to frequently asked questions, including via a new client- and worker-facing website.
Bryan Kutner, PhD, MPH, Albert Einstein College of Medicine
Samuel Anyula Gorigo, Hoymas (Health Options for Young Men on HIV/AIDS and STIs) Kenya
Today — in the US and around the world
There are no words that can adequately, or appropriately, describe the state of the world right now and how AVAC and I are feeling about it. I expect it is a similar sentiment for all of us — irrespective of where we live and vote.
AVAC was founded 30 years ago — in a very different time, with very different political and economic dynamics and epidemiologic realities. But from that beginning, AVAC has always championed an evidence- and rights-based, equitable response to the HIV epidemic — honoring choice and dignity for all.
And we will not stop — not until we are done, and most definitely not now!
We will all need time to process these US election results and strategize how we navigate through them in the days and years ahead — as individuals, as a network of partners, as citizens of the world, and — most importantly — as advocates for choice, freedom, science, and rights.
There will, undoubtedly, be major implications for global health and the global AIDS response. We look forward to working with our partners in protecting hard-fought gains and in assessing the potential impact on PEPFAR and Global Fund support; on USAID, NIH, CDC and the FDA; on the US relationship to WHO and other UN agencies; and on evidence- and rights-based policies and programs generally.
We will be in touch soon with an initial analysis, starting with the release of a podcast next week with Jen Kates from KFF and our own Suraj Madoori as we begin to unpack it all. And we look forward to working with all of you in reviewing it and making it actionable.
Thank you; stay tuned; and stay strong.
Mitchell J. Warren Executive Director AVAC
STIWatch Newsletter, November 2024
The past few months have brought exciting developments in the field of Sexually Transmitted Infections (STIs). The World Health Organization released the global priorities for STIs, which included the need to develop low-cost, rapid, STI point-of-care tests, vaccines, and communication strategies to increase STI awareness, prevention, service engagement. But we continue to see a soaring rise in STI incidence and an underfunded infrastructure for researching new treatment, prevention and testing tools. It’s up to the global community to ensure that research and development continues to see funding for better, faster, less expensive tools to reduce the toll of STIs. Read on for resources and insights to guide your advocacy.
Conference updates
The annual conference of the International AIDS Society in July highlighted the troubling trend in the soaring rise in STI incidence. A preconference, Mobilize for Action on Sexually Transmitted Infections addressed the urgent need to confront the global spike in STI rates, particularly syphilis, gonorrhea, chlamydia, and trichomoniasis. Dr. Jeanne Marrazzo, director of NIAID, when discussing the number of global deaths from syphilis, which is treatable, said, “I think some of the more staggering statistics here, in addition to the sheer number of new infections, is the fact that we had in 2022 over 200,000 syphilis-associated deaths, which to me is practically medieval.” The meeting hosted a rigorous debate exploring the question of implementing DoxyPEP, given there’s no efficacy data for cisgender women in light of fears of creating drug resistant strains of STIs from wider use of doxycycline. Strong arguments were made on both sides, but this controversy is one of the reasons AVAC recently published an Advocate’s Guide to Doxycycline to Prevent STIs.
The STI Prevention Conferencein Atlanta, Georgia convened attendees in-person for the first time in four years and discussed the rise in syphilis rates, emerging gonorrhea treatments, STI funding and policy initiatives, and doxycycline post-exposure prophylaxis (DoxyPEP). Notably, much discussion centered on NIAID’s support for a biorepository to advance diagnostic development. This biorepository would streamline access to necessary specimens to support the research and development of new diagnostics.
Save the date
New resources
Discover STIWatch.org!
STIWatch.org is an updated platform designed to enhance understanding and advocacy for STI vaccine and diagnostics research, development, and rollout. It offers comprehensive information on common STIs, a clinical trials dashboard, advocacy priorities, and a range of resources and tools to support STI prevention and treatment efforts.
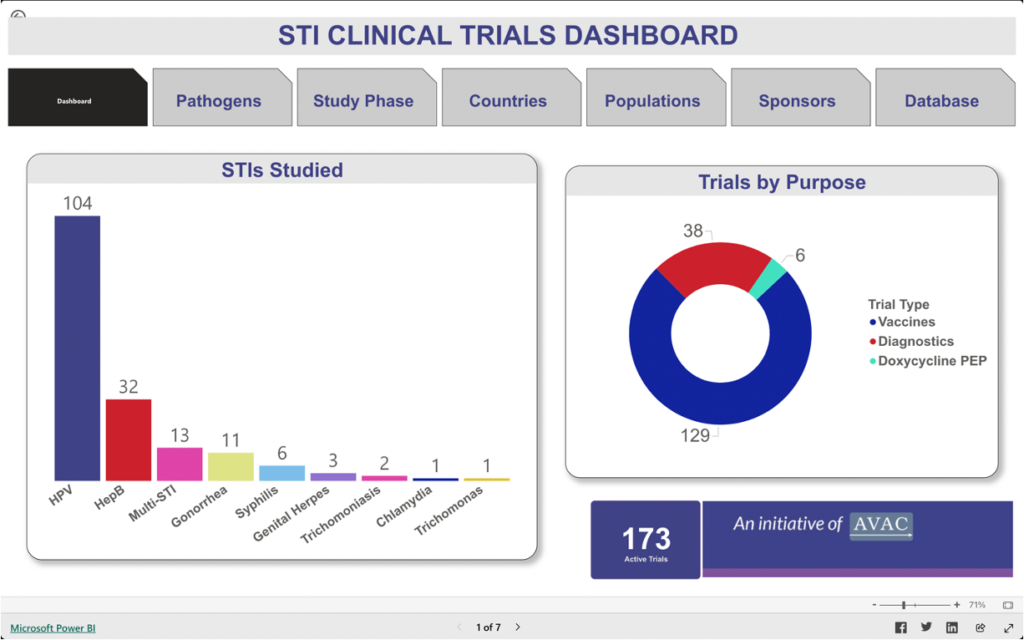
STI Clinical Trials Dashboard
This dashboard provides information about trials focused on vaccines, diagnostics, and the use of doxycycline post-exposure prophylaxis (DoxyPEP) to detect, treat, and prevent chlamydia, gonorrhea, hepatitis B, herpes simplex virus (HSV), human papillomavirus, syphilis, trichomoniasis infections, and Mycoplasma genitalium.
Webinar Summary
Regulatory Pathways to Promote Access to STI Diagnostics. This webinar co-hosted with World Health Organization (WHO) supported researchers, product developers and the global advocacy community in identifying and discussing ways to bring new STI diagnostics to market with speed, equity and scale.
What We’re Reading
Special Issue: Sexually Transmitted Diseases. This leading journal celebrated 50 years by publishing a series of editorials that review the careers of some of the leading experts in the field. These stories are both inspiring and enlightening, highlighting the decades of efforts and growth in addressing STIs. AVAC’s own, Alison Footman, PhD, wrote about her experiences in the STI field and how instrumental mentorship has been in her career growth.
Gonorrhea point-of-care diagnostics technology and market landscape. This landscape report provides an overview of gonorrhea point-of-care diagnostics that can be offered closer to patients and communities and limit time to results and ultimately treatment. Gonorrhea touches on multiple public health priorities including the need to reduce STI rates, growing antimicrobial resistance, and its impact on sexual and reproductive outcomes and HIV transmission.
FDA Marketing Authorization Enables Increased Access to First Step of Syphilis Diagnosis. The US Food and Drug Administration approved the first syphilis self-test. This is a monumental step in expanding syphilis testing options as infections have increased drastically over the past five years. Self-tests can provide people with the option to learn their syphilis status and seek additional testing and treatment options from a healthcare provider.
Partner Spotlight
AVAC partners have been busy moving the needle to improve STI prevention, testing, and treatment options in their respective countries. The Latu Human Rights Foundation partnered with HEP Initiative Zambia on a symposium to foster ideas on how to better address viral hepatitis and integrate hepatitis B interventions into other government funded health programs.
The past few months have brought exciting developments in the field of Sexually Transmitted Infections (STIs). The World Health Organization released the global priorities for STIs, which included the need to develop low-cost, rapid, STI point-of-care tests, vaccines, and communication strategies to increase STI awareness, prevention, service engagement. But we continue to see a soaring rise in STI incidence and an underfunded infrastructure for researching new treatment, prevention and testing tools. It’s up to the global community to ensure that research and development continues to see funding for better, faster, less expensive tools to reduce the toll of STIs. Read on for resources and insights to guide your advocacy.
Conference updates
The annual conference of the International AIDS Society in July highlighted the troubling trend in the soaring rise in STI incidence. A preconference, Mobilize for Action on Sexually Transmitted Infections addressed the urgent need to confront the global spike in STI rates, particularly syphilis, gonorrhea, chlamydia, and trichomoniasis. Dr. Jeanne Marrazzo, director of NIAID, when discussing the number of global deaths from syphilis, which is treatable, said, “I think some of the more staggering statistics here, in addition to the sheer number of new infections, is the fact that we had in 2022 over 200,000 syphilis-associated deaths, which to me is practically medieval.” The meeting hosted a rigorous debate exploring the question of implementing DoxyPEP, given there’s no efficacy data for cisgender women in light of fears of creating drug resistant strains of STIs from wider use of doxycycline. Strong arguments were made on both sides, but this controversy is one of the reasons AVAC recently published an Advocate’s Guide to Doxycycline to Prevent STIs.
The STI Prevention Conferencein Atlanta, Georgia convened attendees in-person for the first time in four years and discussed the rise in syphilis rates, emerging gonorrhea treatments, STI funding and policy initiatives, and doxycycline post-exposure prophylaxis (DoxyPEP). Notably, much discussion centered on NIAID’s support for a biorepository to advance diagnostic development. This biorepository would streamline access to necessary specimens to support the research and development of new diagnostics.
Save the date
New resources
Discover STIWatch.org!
STIWatch.org is an updated platform designed to enhance understanding and advocacy for STI vaccine and diagnostics research, development, and rollout. It offers comprehensive information on common STIs, a clinical trials dashboard, advocacy priorities, and a range of resources and tools to support STI prevention and treatment efforts.
STI Clinical Trials Dashboard
This dashboard provides information about trials focused on vaccines, diagnostics, and the use of doxycycline post-exposure prophylaxis (DoxyPEP) to detect, treat, and prevent chlamydia, gonorrhea, hepatitis B, herpes simplex virus (HSV), human papillomavirus, syphilis, trichomoniasis infections, and Mycoplasma genitalium.
Webinar Summary
Regulatory Pathways to Promote Access to STI Diagnostics. This webinar co-hosted with World Health Organization (WHO) supported researchers, product developers and the global advocacy community in identifying and discussing ways to bring new STI diagnostics to market with speed, equity and scale.
What We’re Reading
Special Issue: Sexually Transmitted Diseases. This leading journal celebrated 50 years by publishing a series of editorials that review the careers of some of the leading experts in the field. These stories are both inspiring and enlightening, highlighting the decades of efforts and growth in addressing STIs. AVAC’s own, Alison Footman, PhD, wrote about her experiences in the STI field and how instrumental mentorship has been in her career growth.
Gonorrhea point-of-care diagnostics technology and market landscape. This landscape report provides an overview of gonorrhea point-of-care diagnostics that can be offered closer to patients and communities and limit time to results and ultimately treatment. Gonorrhea touches on multiple public health priorities including the need to reduce STI rates, growing antimicrobial resistance, and its impact on sexual and reproductive outcomes and HIV transmission.
FDA Marketing Authorization Enables Increased Access to First Step of Syphilis Diagnosis. The US Food and Drug Administration approved the first syphilis self-test. This is a monumental step in expanding syphilis testing options as infections have increased drastically over the past five years. Self-tests can provide people with the option to learn their syphilis status and seek additional testing and treatment options from a healthcare provider.
Partner Spotlight
AVAC partners have been busy moving the needle to improve STI prevention, testing, and treatment options in their respective countries. The Latu Human Rights Foundation partnered with HEP Initiative Zambia on a symposium to foster ideas on how to better address viral hepatitis and integrate hepatitis B interventions into other government funded health programs.
Join the Fight Against HIV: Discover the latest breakthroughs
Are you passionate about medical breakthroughs and advocacy? Don’t miss out on this pivotal community event where leading scientists and dedicated advocates gather to discuss with you the latest strides in HIV cure research.
Meet Two People Cured of HIV: Hear their stories, learn about their journeys, and discover the breakthroughs in medical science that made their cures possible. This is a unique opportunity to gain insight into the advancements in HIV and the hope it brings to many.
Explore Cutting-Edge Research: Get insights into the latest advancements towards finding a cure for HIV. Hear directly from the experts who are at the forefront of this critical work.
Engage in Thought-Provoking Discussions: Participate in conversations that matter. Share your thoughts a cure for HIV and learn from others who are just as committed to this cause.
Network with Like-Minded Individuals: Connect with those who share your dedication to making a difference. Build relationships that could shape the future of HIV advocacy and research.
Be Inspired to Take Action: Leave feeling motivated and equipped with new knowledge to contribute to the fight for a cure for HIV in meaningful ways.
Since 2019, rates of HIV acquisition in Latin America have been trending upward, from 110,000 annually in 2019 to approximately 120,000 in 2023. At the same time, Latin America has taken strides to combat this trend, from increasing PrEP initiation rates to preparing for longer acting PrEP products, such as injectable cabotegravir (CAB) and lenacapavir (LEN). Learn more in PxWire.
Avac Event
True Choice in HIV Prevention Involves More than Product Options: Novel strategies in service delivery
The Choice Agenda and presenters from Brazil, Kenya, and South Africa discussed novel strategies for the delivery of HIV prevention interventions. All HIV prevention products have their “Achilles Heels.” Differentiated service delivery supports reaching a wide range of potential users and can overcome challenges with product attributes. Offering different strategies can also make the interface with health care easier and more community friendly.
Speakers:
Ines Dourado, Universidade Federal da Bahia
Catherine Verde Hashim, AVAC
Catherine Martin, Wits RHI
Katrina Ortblad, Fred Hutch
Adriano Queiroz, City of São Paulo Municipal Health Secretariat
Daniel Were, Jhpiego
Thanks to WHO for providing live simultaneous Ukrainian translation and to PAHO for providing live simultaneous translation in Portuguese and Spanish.
PIBA Presents Reimagining the HIV Prevention Blueprint for Black Communities in Arkansas, Mississippi, and Tennessee
PrEP in Black America (PIBA) with regional Partners will host a Virtual Town Hall titled, Reimagining the HIV Prevention Blueprint for Black Communities in Arkansas, Mississippi, and Tennessee.
This is designed to offer a virtual platform for leaders in Mississippi, Tennessee, and Arkansas to share the narrative of PrEP within Black communities. The town hall will concentrate on three main objectives: 1. Motivating the Black public health workforce to spearhead the public health response. 2. Educating the broader Black community about the science and efficacy of PrEP. 3. Advocating for a federally funded national PrEP program.
Local Partners Include:
Community Health-PIER (MS)
FABRIC, Incorporated (MS)
Mississippi AIDS Education and Training Center (MS)
WeCare TN
Ryan White Part A Program Memphis (TN)
PIBA requests that only residents of Mississippi, Tennessee and Arkansas (US) attend this virtual town hall.