Three HLMs, A Host of Challenges and One Major Victory
For the last year, reforming the global health architecture in the hopes of delivering health more equitably has been top of mind. From the Pandemic Fund launch, to post-mortems on the ACT-A (the global body convened to develop COVID-19 interventions and ensure access to them), to the call for a new Pandemic Accord, a strong consensus had finally emerged that things need to change.
Accordingly, this theme ran throughout the health-related proceedings at the UN General Assembly in September where High-Level Meetings (HLMs) on universal health care (UHC), Tuberculosis (TB), and Pandemic prevention, preparedness and response (PPPR) took place.
Four key takeaways from the week stand out to AVAC:
Multilateralism is threatened. Tensions between countries are incredibly high. Each day’s proceedings made clear that the spirit of diplomacy from previous years has waned. Given that there have already been UN Declarations on UHC and TB, advocates went into this year’s process thinking that stronger declarations would be relatively easy to negotiate. But countries were at odds during negotiations for all three health-related HLMs. Country representatives disagreed on a host of issues that will impact access to medical products, financing, and who is responsible for addressing health crises. These disagreements upended usual procedure. Typically, the Declaration is finalized weeks before the actual HLM; this year, a final decision on all three Declarations hung in the balance until the minute before the meetings began. Advocates must work hard in the coming year to bring countries together on key issues in the Pandemic Accord.
Access is THE issue. By far, the question of access to medical products and tools dominated all three HLMs. Tensions around this issue sparked the most heated disagreements during negotiations. During the PPPR HLM, Member States speaking from the UN floor all mentioned their commitment to building more equitable access to medical countermeasures, but richer countries are unwilling to alienate the pharmaceutical industry by including access commitments in international agreements. And lower-income countries are refusing to permit open access to data on new pathogens without access commitments to the products derived from that data. The issue is so fraught it almost derailed any health Declarations at all. Right before HLM week, eleven countries that have been the target of ‘unilateral coercive measures’ (sanctions) sent a letter to the President of the General Assembly refusing to sign on to the declarations because the sanctions prevent them from accessing medical countermeasures — tools, medicines and equipment, needed in a health crisis. The Declarations ended up moving forward anyway with very limited commitments on how best to ensure access to medical countermeasures. It will be imperative for advocates to keep the issue of access front and center and help to navigate toward agreements that all countries can stomach.
Civil society engagement is going backward. The PPPR HLM had no civil society formal engagement mechanism, and the process suffered because of it. Civil society was left out of the loop. They didn’t receive information about the status of negotiations, or details on sticking points. These updates would typically be funneled through a formal mechanism. In addition, the HLM process usually includes two to three days of Multistakeholder Hearings for each HLM to allow civil society to state their priorities and views ahead of negotiations on the draft Declaration. This year, each HLM had just one half-day, significantly limiting the number of civil society organizations and advocates that could get their views in front of Member States. Approvals for registration for both the Multistakeholder Hearings and HLMs came less than a month before the actual event, leaving many advocates too little time to get visas to the US. To add insult to injury, during the HLM, many civil society advocates did not get to make statements from the floor even though time was reserved for civil society – agencies such as Gavi and the Global Fund and pharmaceutical corporations spoke during these slots. Engagement with UN staff is needed to better define what constitutes civil society, and to protect these rare points of access and influence for those who speak for communities.
Policymakers are starting to understand the contributions HIV, TB, and malaria can make to pandemic preparedness. As the furor to address huge gaps in pandemic preparedness and response capacities ramped up in 2021, it was a slog to get policymakers new to the space, who had not traditionally been involved in health negotiations, to understand the underlying infrastructure and movements that the global responses to HIV, TB, and malaria have built. However, this year’s UN General Assembly showed that advocates have made a lot of progress. The Coalition of Advocates for Global Health and Pandemic Preparedness, of which AVAC is a co-founder, pushed hard for inclusion of these ongoing pandemics in the Declaration on PPPR to great success – two clauses recognizing the existing infrastructure from these responses that can be leveraged for pandemic preparedness and committing to continue the fight to end these ongoing pandemics made it into the final Declaration text. Much more needs to be done to harmonize the PPPR and HIV/TB/malaria architecture, saving advocates and everyone involved in pandemic preparedness extensive time and resources, but the recognition of the interconnectedness of future and ongoing pandemics represents a huge win.
At AVAC, we have put a lot of hope in the processes of the Pandemic Accord, the UN High-Level Meeting (HLM) on Prevention, Preparedness, and Response (PPPR), and the development of a medical countermeasures (MCM) platform. To understand how these three efforts fit together, see AVAC’s Advocate’s Guide to PPPR.
Sam Rick authored a piece, Who’s Driving this Ship, which takes a critical look at the issues challenging Global North governments in creating a system that is equitable and aims to prevent health threats everywhere and prepare everyone.
PPPR Advocacy 101: Find out what it means to you: For a deep dive on the diverse initiatives aimed at preparing for the next pandemic. Learn what they commit to, how much they will spend, and how well these plans incorporate equity as a principle.
In recent weeks, important new resources for advancing choice in HIV prevention have been announced. Don’t miss these highlights from the field. They point to an HIV response in transition, and help to define the role advocacy must play. As policy, practice and budgets strive to keep up with advances in research, advocacy around choice becomes a cross-cutting priority—so that the promise of new options in HIV prevention won’t be squandered in siloed programs, or by poorly-planned supply chains, or because of disconnected policy decisions. People have diverse needs and face complex challenges; ending HIV depends on finding the option that works best for each individual.
The Choice Manifesto
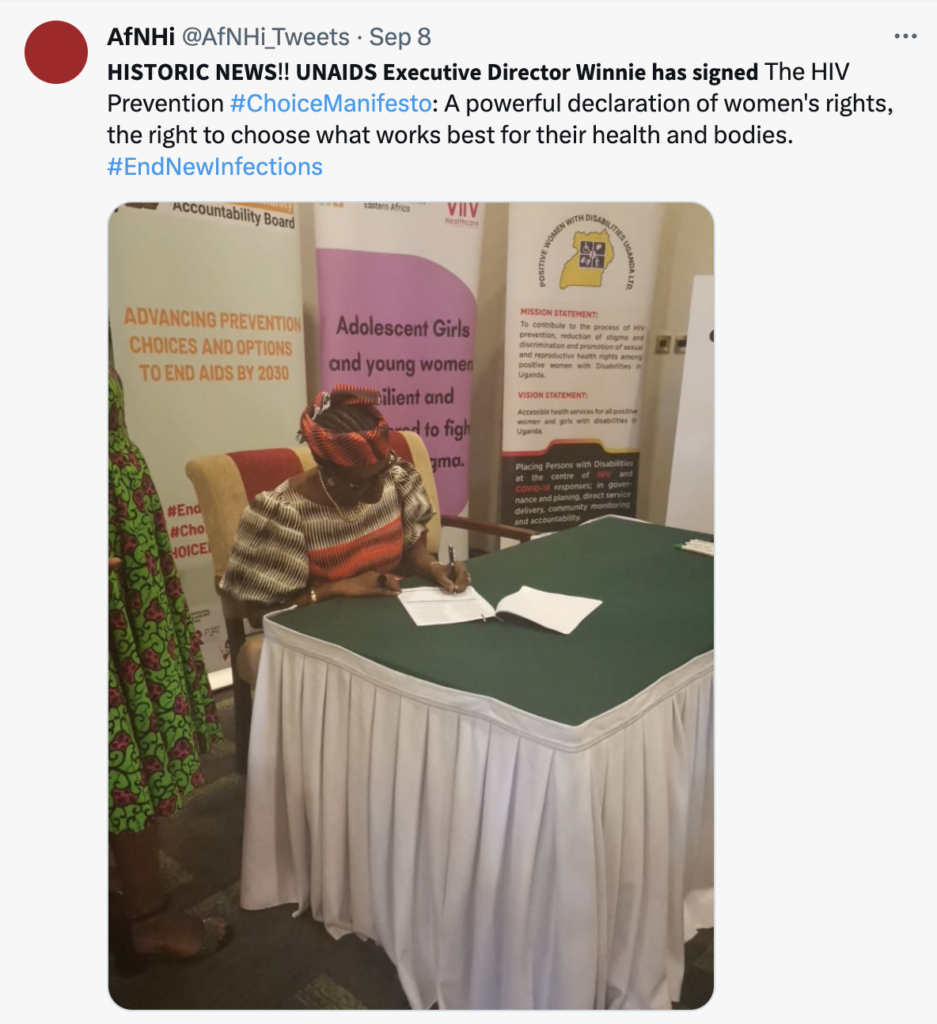
The African Women’s HIV Prevention Community Accounability Board (AWPCAB) launched the HIV Prevention Choice Manifesto, calling for increased political and financial support to ensure every proven method of HIV prevention is integrated into the HIV response, so that all women who need prevention will have access to the options that will make prevention possible for them. At the launch event in Kampala, UNAIDS Executive Director Winnie Byanyima gave a keynote address in support of the Manifesto’s call for all stakeholders to commit to the budgets and strategies that will make choice possible.
“I congratulate you for the HIV Prevention Choice Manifesto. It’s about pushing everyone towards people-centered, women-centered and women-led approaches to HIV prevention. You have fought with your lives to get here. You are fearless feminists. Women must lead for themselves.” – Winnie Byanyima, UNAIDS Executive Director
The DPP Consortium created a multiyear strategy to frame priorities and next steps in the development and delivery of the dual prevention pill (DPP), which is being developed to prevent HIV and unintended pregnancy. This multipurpose prevention technology (MPT) combines oral PrEP with an oral contraceptive. The updated strategy consolidates two years of progress toward preparing the field for new MPTs. The strategy addresses additions to the MPT pipeline, the potential role of the private sector in delivering a future DPP, recommendations for provider counseling on the use of the DPP, market research on potential DPP users, the latest analysis on cost, and more.
Stay tuned for more resources and updates to come on the DPP, the Choice Manifesto, and tools for connecting choice to HIV prevention, ending the epidemic and the role of choice in global health equity in HIV, and beyond.
Reclaiming Choice: The launch of the HIV Prevention Choice Manifesto and what that means
The African Women’s HIV Prevention Community Accountability Board (AWCAB) launched its HIV Prevention Choice Manifesto in Kampala, Uganda on September 8, 2023. This document, and the advocacy behind its development and release, marks a historic milestone in the power of community-led leadership and prioritization of choice in HIV prevention.
“The toolbox for HIV prevention products is still falling short. More options are needed to suit everyone at different stages of their lives including an effective, accessible, and safe HIV vaccine if we want to see an end to the epidemic”. – Joyce Ng’ang’a, WACI Health, Accountability Board Member and Communications Lead
The AWCAB is a coalition of women and girls living and working in Africa who are united in calling for continued political and financial support for more choice in HIV prevention through the HIV Prevention Choice Manifesto. This comes at a time when political will and financial investment are critical to deliver new prevention options such as CAB for PrEP and the dapivirine vaginal ring to meet the needs of women and girls in Africa. In 2023, over four decades in the epidemic, a vast array of biomedical tools to prevent HIV acquisition exist, but these tools are only effective in their purpose if there is universal access, if communities know they exist and are able to choose from all the available options. The manifesto serves as a declaration of what could happen if African women and girls not only had a seat at the table, but led the response and advocacy efforts that shape healthcare for HIV prevention.
“We have come a long way in the fight to secure choice in HIV prevention for women and girls. We are at a watershed moment to ensure we close the gap for new infections among women and girls. The launch of the Choice Manifesto is the beginning of the work ahead of us as we call on key players to sign onto the manifesto and become part of the change.” – Yvette Raphael, Advocacy for Prevention of HIV and AIDS (APHA), Accountability Board co-chair
Most notable was the presence of UNAIDS Executive Director, Winnie Byanyima, who delivered the keynote address and publicly endorsed and signed the Manifesto. Key stakeholders in HIV prevention participated in the launch and affirmed their commitments to choice. This included leadership from UNICEF, UN WOMEN, ViiV, PEPFAR, USAID, Global Fund, Ministry of Health, Uganda, Population Council/ IPM, Aidsfonds, FHI 360 and other civil society organizations. The commitments leadership and key stakeholders signed were focused on elevating national and global dialogue, ensuring resources to prevention options were accessible and sustainable, and bolstering support for local manufacturing of prevention products. Following the launch of the Manifesto, UNAIDS released a feature story on its website HIV Prevention Choice Manifesto for Women and Girls in Africa launched, highlighting the commitment to choice.
Explore resources, tools, and takeaways from the launch including the full HIV Prevention Choice Manifesto.
“The Choice Manifesto is an important and timely advocacy tool. It will help advocates lobby for resources and political will towards making HIV prevention options available for women and girls in Africa. We need commitment and actions from all stakeholders including funders and governments towards CHOICE-based HIV Prevention Programming”. – Grace Kumwenda, AVAC, Accountability Board Member
AVAC stands in solidarity with the Accountability Board, and congratulates the group on this major advocacy win! AVAC reaffirms its ongoing commitment to support the Accountability Board as part of the Coalition to Accelerate and Support Prevention Research (CASPR) and to champion the cause of ensuring choice in program implementation, access to and procurement of prevention options; and to advocating that the prevention agenda is shaped by women and girls who seek and want these essential tools.
“We are not asking for much! Let us stop being comfortable with shameful statistics of alarming new HIV infections among adolescent women and girls and start providing options for HIV prevention that meet their needs. Their lives matter!” – Lillian Mworeko, International Community of Women living with HIV Eastern Africa (ICWEA), Accountability Board co-chair
As advocates continue to track and translate HIV prevention tools on the horizon, including already existing and revolutionary long-acting medications, it is important to listen to those who are leading the fight for equity and center choice in all of our implementation efforts.
PEPFAR is one of the greatest US foreign policy and global development achievements of the century. The program has saved upwards of 25 million lives since it launched in 2003. But as PEPFAR marks its 20th anniversary, it’s also fighting for its future.
The US Congress needs to reauthorize PEPFAR for another five years by September 30 and reaffirm its commitment to this lifesaving program. Until a couple of months ago, most in global health and development expected smooth sailing for a five-year reauthorization of the program, as has happened throughout the past 20 years. PEPFAR has enjoyed deep and broad bipartisan support since its founding. Evangelical Christians, staunch conservatives and progressive liberals, Democrats and Republicans, HIV activists, civil society advocates and public health leaders have all championed PEPFAR, year in and year out. But a handful of Republicans, including past PEPFAR allies, are pulling reauthorization into high-stakes partisan politics.
In this episode, Px Pulsetalks to some of the people who put PEPFAR dollars into action and to global health leaders who explain why PEPFAR’s approach has been so effective, and what’s at stake in this debate.
Tune in to hear:
Ilda Kuleba from Mothers 2 Mothers talks about the impact of PEPFAR on their work across 10 countries, training and employing HIV positive mothers as peer healthcare workers.
Dr. James Mukabi of World Vision’s Kenya program talks about how this Christian relief organization has changed the lives of thousands of orphans and other populations who are vulnerable to HIV.
Tom Hart, President of the ONE Campaign, which was co-founded by the rock star Bono, to be an early champion of PEPFAR and other poverty fighting efforts talks about PEPFAR’s accomplishments at the global level and what’s next as Congress debates reauthorizing the program.
PEPFAR’s supporters have a job to do, to make sure everyone understands that the world has a lot to lose if PEPFAR is weakened and so, so much to gain if US policymakers unite in their support. We hope you will listen and pass on the episode, download the resources and, most especially, add your voice in support of PEPFAR.
The updated AVAC.org also reflects the expanded vision and practice of our dynamic programs. AVAC will always work to accelerate ethical development and equitable delivery of effective HIV prevention options. But, we also know that responding to HIV and preparing for future pandemics requires a comprehensive, integrated, and sustained response that is rights-based, people-centered and evidence-informed.
To AVAC, this means connecting the dots between HIV prevention, sexual and reproductive health and rights, pandemic preparedness, strengthened health systems, research engagement and community leadership. It means recognizing that resilience in global health requires us to confront the threats posed by disparities in access, entrenched stigma, discrimination, criminalizing key populations and inadequate responses to other sexually transmitted infections.
Visit the new AVAC.org for resources, tools and analysis that make these connections as we continue to track and translate the field, including:
Information on the entire pipeline of biomedical prevention strategies being investigated today
Our projects, which showcase the incredible partnerships and collaboration that underpin everything we do
Our podcast, PxPulse, which will deepen your knowledge and help you “check the pulse” of this fast-paced field and the urgent challenges still ahead
PxWire our quarterly update on where we are in biomedical prevention research
Our HIV clinical trials database, where you can find details on all biomedical prevention trials and our broader resource database containing fact sheets, infographics, blog posts and more on HIV prevention and the broader issues surrounding global health equity
We are immensely proud to share these resources with you. We hope these tools and analyses will help to power your advocacy, accelerate ethical development and equitable delivery of effective HIV prevention options, and advance global health equity.
Achieving successful HIV prevention relies on programs and research shaped by communities and grounded by their needs and priorities. Skilled and informed community advocates drive this process. AVAC’s Advocacy Fellows Program expands and strengthens the capacity of civil society advocates and organizations to monitor, support and help shape HIV prevention research and rapid rollout of new effective interventions in low- and middle-income countries facing substantial HIV burdens.
The program provides intensive support to emerging and mid-career advocates to execute advocacy projects addressing locally identified gaps and priorities. Fellows receive comprehensive training, financial backing, and technical assistance to strategize and execute a targeted 18-month project hosted by an organization within their country.
In its 15-year history, 85 Fellows and 75 partner organizations across 15 countries have participated in the program. They have influenced policy, championed community perspectives, strengthened healthcare systems, demystified HIV prevention research, advocated for fairness and transparency on local, regional, and global scales and now lead many national and regional organizations. Discover more about the program’s impact here. As the 2022 Fellows conclude their Fellowships, learn more about their projects and achievements here.
What’s New in 2024
While HIV biomedical prevention advocacy remains central, we encourage projects with a strong focus on health equity, structural considerations, and links to TB, STIs, and sexual and reproductive health and rights. Advocacy projects related to pandemic prevention, preparedness and response are also welcomed.
Eligibility
Emerging or mid-career community leaders and advocates who want to advance their advocacy skills and advocate for HIV, SRHR, STI, TB, and pandemic prevention and preparedness.
Individuals with experience or education in HIV or public health, or in advocacy for key populations (e.g., sex workers, LGBTQIA+ individuals, pregnant individuals, people who use drugs) or for social and economic justice.
Based in low- and middle-income countries with substantial HIV burdens and ongoing HIV prevention research or introduction of new interventions.
Please note that for 2024 fellowships, priority focus lies in Eastern and Southern Africa.
Applications are due by 2 October 2023, and 2024 Fellowships will run from April 2024 through September 2025.
Spread the Word
Help us reach potential advocates by sharing this information within your networks.
We look forward to receiving your application and making a positive impact together.
From Brisbane to Chicago: A look at STIs, HIV and global health
Late July saw two nearly simultaneous conferences on the future of research and advocacy for HIV and sexually transmitted infections (STIs). IAS 2023 in Brisbane and the 2023 STI and HIV World Congress (also known as ISSTDR) in Chicago are landmark annual events. Both conferences bring together civil society, advocates, policy makers, donors and scientists to share the latest scientific findings and discuss where advocacy is needed to both advance research and ensure equity informs every aspect of the development process, from basic science to delivering new interventions. There may be two gatherings, but it’s one vital conversation. HIV and STIs are inextricably linked, affecting the same communities, who face the same barriers to care and prevention against these health threats. At AVAC, we see the links and we are making the connections. Below we offer highlights from these two all-important world gatherings, and check out our recent webinar linking these conversations, Tales from Two Cities: HIV and STI research highlights from Brisbane and Chicago.
This satellite, co-sponsored by PATH, IAS, WHO and AVAC, put a spotlight on integrated, person-centered care, a central theme of the 2023 UNAIDS report launched at IAS 2023, The Path That Ends AIDS. UNAIDS reports that investing in person-centered priorities such as community-led services, integrating primary health care with HIV services, and a strong health workforce brings down incidence. And the pressure to scale up these approaches remains essential. According to the latest statistics in the report, only 42% of districts in African countries with very high HIV incidence are covered by prevention programs. Even more chilling, 4,000 adolescent girls and young women acquire HIV every week.A presentation in this session by former AVAC Fellow and CASPR partner Chilufya Kasanda from Zambia’s TALC put a face and a voice to this story. In Zambia, youth friendly services are scarce or non-existent, high rates of mental health issues are utterly neglected, and donors “flock to a few locations and leave out those who are most in need.” She said community advocates are too often dismissed as “people just making noise.” But, said Chilufyia, it’s young people who must receive support, their leadership must be nurtured and funded, and messages should be tailored just for them. “Young people need to know that pleasure, not only risk, is attached to sex. To get to pleasure, you need to be safe, that is the message.” Another AVAC Fellow, Elizabeth Onyango from Kenya’s Coast Sex Workers Alliance, called for accelerating access to the dapivirine vaginal ring. “Why is the ring not in our vaginas? Male condoms even come in different flavors! This is a women-first product and it needs more investment.”
Prevention will fail if the HIV response remains narrowly focused on products. Oral PrEP has brought invaluable lessons we have yet to learn about how to get programming right so that effective products actually reach those who need them. As AVAC Executive Director Mitchell Warren said at the conference, reflecting on the status of PrEP uptake since FDA approval in 2012- “Only 4m global PrEP initiations in 12 years is an epic failure. Science has given us products that work, but our policies and programs have failed to meet the needs.”
This session featured presentations from AVAC on a package of tools called, Getting Rollout Right and the work of the Coalition to Accelerate Access to Long-Acting PrEP. Daniel Were of Jhpiego talked about lessons from the Jilinde project, Kenya’s ambitious program to deliver PrEP. The project adapted in real time to reach more people by recognizing that peer networks are essential, that stopping and starting PrEP is common, and that provider attitudes can be difficult to change. Daniel stressed the importance of focusing deeply on the people who need to use these products.
This preconference forum on HIV cure research featured innovative presentations tracking the progress toward an HIV cure. AVAC Senior Program Manager Jessica Salzwedel participated in a panel discussion on the importance of increasing diversity throughout HIV cure research from trial participants, to advocates, to researchers. The session also featured the release of a new resource on community preferred language for HIV cure.
This session covered the potential for research on broadly neutralizing antibodies (bNAbs) to inform strategies for both prevention and cure. AVAC partner Maureen Luba joined the panel discussion to applaud collaboration among the bNAb researchers working in prevention and cure, and she called for the same collaboration with communities. She said research budgets for community engagement should reflect the importance of community leadership right from the beginning, to ensure success in the future. Maureen added “thinking about cost and choice is the elephant in the room. The resource envelope for HIV prevention is not expanding enough. Countries will be asking ‘where will we get the money [for bNAbs].’ We have to think about cost effectiveness now.”
Investigators and advocates discussed innovative methods to test how new interventions compare to oral PrEP, and how to also make comparisons to HIV incidence in a given community. Models of community engagement were just as important in the conversation. Ntando Yola of APHA described robust programs that brought community members along as these complex new trial designs were developed. Investing in Good Participatory Practicemeans investing “in the platforms that equip and empower communities and advocates,” said Ntando. And for more on how trial design is evolving, check out AVAC’s Evolving Designs for HIV Prevention Trials.
AVAC at the STI & HIV World Congress
The STI Prevention Pipeline: Where Are We, and What Will It Take to Move Forward Faster?
This session on the state of the field offered updates on how STI prevalence and incidence rates are estimated, STI vaccine acceptance, STI test development, and information on the first US STI National Strategic Plan and Federal Implementation Plan. The session included discussions about advocacy priorities in each of these areas, with discussions continuing in the Advocacy Zone throughout the conference (see below). For more on the STI pipeline, check out the resource pages on STIwatch.org.
Setting Up a Remote/Home Testing STI Programme: A Practical Toolkit
This session explored the power of remote testing to curb STI acquisitions. Remote and home-testing brings many benefits. It’s convenient, overcomes barriers from stigma, offers privacy, reflects trauma-informed principles, and can overcome structural barriers. For the status of testing for several STIs go to the pathogen pages on STIwatch.org.
Symposium: New Vaccine Approaches to STI Prevention, STI Vaccine Acceptance, and Equity
This symposium shared progress on STI vaccine research and examined the question, “what factors could influence acceptance of STI vaccines and how do we ensure equitable access to these vaccines”. AVAC’s Dr. Alison Footman referenced the disparities in the COVID-19 vaccine and how vaccine access can differ due to income, health insurance, and region. Considerations around equity, access, vaccine hesitancy, vaccine confidence, and vaccine awareness must be confronted as an integrated part of the advocacy for STI vaccine development. This session provided a platform for framing these issues and developing an agenda for advocacy.
ISSTDR Advocacy Zone
AVAC hosted an Advocacy Zone at the conference, which bubbled with activity throughout the meeting. Advocates used this space to weigh in on questions and share perspectives on how the STI field can grow and how advocacy can equitably advance the field. Overall themes included the need to normalize sexual health, center pleasure in STI conversations and the urgency for increased funding to support STI prevention and research.
Spotlight on WHO News at Both Conferences
The WHO made headlines from Brisbane and Chicago, with major announcements and research findings that will be shaping global health for years to come. U=U and Zero Risk
Also from Brisbane, the WHO announced new HIV testing guidelines, calling for countries to expand use of HIV self-testing (HIVST) and to promote testing through social networks. In a July 22 press release, the WHO said, “These recommendations are issued at a moment of unique opportunity, when self-care and self-testing are increasingly being recognized as ways to increase access, efficiency, effectiveness and acceptability of health care across many different disease areas, including HIV.”
Surveillance of Mpox
The WHO presented their mpox surveillance data in Brisbane, building on findings reported at the Conference of Retroviruses and Opportunistic Infections that showed mpox severely impacts people living with HIV (PLHIV) who have a very low CD4 T-cell count. The WHO analysis draws from a larger set of data than was presented at CROI, and it found PLHIV with advanced immunosuppression were twice as likely to be hospitalized than people who are HIV-negative. See the aidsmap article for details.
Women Want CAB for PrEP as a Choice in HIV Prevention
Researchers presented findings from the open label extension study of HPTN 084 studying injectable cabotegravir (CAB) for PrEP, among individuals born female. Among 2500 participants in seven African countries, nearly 78% chose injectable CAB and 22% preferred oral PrEP. And a related study, HPTN 084-01, also found CAB for PrEP was generally acceptable to a small study of cisgender adolescent women in a study conducted in South Africa, Uganda and Zimbabwe. 92% opted to continue use of CAB for PrEP in the open label extension. The study also found that engagement of parents or guardians could be pivotal, providing young women with the support they need to make choices with confidence. The HPTN’s Erica Hamilton said the study reinforces how much choice matters. “The efficacy of CAB for PrEP was reassuring, but some participants still preferred the oral tablet [which also has very high efficacy] for various reasons.”
New Data on VMMC Among Gay Men and Other Men Who Have Sex with Men (MSM)
A small but noteworthy study from eight cities in China showed VMMC offered protection against HIV transmission among MSM. Researchers say this first randomly controlled trial demonstrating efficacy among MSM should be followed up by larger trials.
Tracking the Inclusion of Transgender People in Research
The launch of AVAC and the Office of HIV/AIDS Network Coordination’s (HANC) Clinical Trial Scoring Tool, provided an initial analysis of the inclusion of transgender people in HIV research and a tool for tracking inclusion in the future. This tool generated great excitement during the poster session. The score card evaluating HIV research since 1991 found less than 1% of participants in 41 key HIV studies included transgender populations. “Dozens of attendees from Harare to Montreal to Hyderabad had questions and expressed interest in using the scorecard and applying it to other populations, too.”
Cure at IAS 2023
The “Chicago Patient” was first presented at CROI 2023 and is the first known case of rebound from a bone marrow transplant where the donor did NOT have a critical and rare mutation to what is called the CCR5 receptor, which is found on certain human immune cells. The individual decided to go back on therapy after two consecutive detectable viral loads. This case is interesting because it suggests that reservoir cells may persist even after extreme clearance measures that are part of a stem cell transplant.
The “Geneva Patient” is the potential sixth cure for HIV. This individual received a bone marrow transplant from a donor with wild type CCR5 — meaning they did not have natural immunity to HIV. The individual experienced severe graft vs. host disease, a complication where the new immune system attacks the host. No virus can be found 20 months off therapy using the most sensitive assays. The medication used to stop the effects of graft vs. host disease promotes latency, meaning the reservoir cells have a harder time reactivating. Researchers are excited about this case because it provides clues on the role of the immune system in clearance and potential pathways toward an HIV cure.
The 5 cases of pediatric control were presented by Gabriela Chaumet of University Kwa Zulu-Natal. This longitudinal study followed 281 mother-infant pairs with in utero transmission. The children were started on ART soon after birth and about 92% were exposed to ART in utero through the placenta. Five of the children, all male at birth, who were not adherent to ART were able to control the virus below detectable levels without therapy. However, Only 40% of the infant cohort was male. The study suggests the importance of the virus itself and indicates the need to further understand the impact sex & gender may have on future HIV cure strategies.
STI Research Highlights
GPP on the STI Map
From two different sessions in Chicago, a GPP champion and San Francisco’s Bridge HIV medical director Dr. Hyman Scott called out the power of Good Participatory Practice. In sessions on Biomedical Prevention for STIs and HIV and Addressing the HIV and STI Syndemic, Hyman’s presentations called for GPP to be implemented broadly. “I am really glad to see AVAC at this conference. We need GPP to hold us accountable,” said Hyman. CASPR partner Zinhle Sokhela of Wits RHI also gave background on GPP during the session Centering Equity, Inclusion and Diversity in STI/HIV Research and referenced a Cameroon and Cambodia PrEP trial that ended prematurely due to lack of effective community engagement. “The [GPP] guidelines help prevent misunderstanding and miscommunication among researchers and stakeholders.”
Antimicrobial Resistance and New Drugs in the Pipeline
Resistance to existing antibiotics for different STIs is spurring a hunt for alternative drugs. The conference presented encouraging early findings on new interventions for herpes simplex virus (HSV) and mycoplasma genitalium (M. genitalium), which cause urethritis and other diseases. A retrospective review of data from 165 patients found minocycline cured 2/3 of the resistant cases of M. genitalium. Phase II studies of pritelivir demonstrated superiority over the standard of care for resistant cases of HSV.
Women and DoxyPEP
Dr. Jenell Stewart presented additional data on the DoxyPEP study out of Kenya and found, from hair testing analyses, that 44% of women assigned to DoxyPEP may have not taken any of the medication. This could be one reason why DoxyPEP has not shown efficacy among women, from data that was previously presented at CROI 2023. Watch this space for more data coming out of the D-PEP Kenya study, including a look at the correlation between PrEP and DoxyPEP adherence, as well as conversations about future research of DoxyPEP in cisgender women.
The Promise of Self-Testing
A presentation by Preventx, a UK-based supplier of self-testing kits, featured their analysis that remote/home-testing led to the diagnosis of a similar number of STIs as those diagnosed in the clinic. Preventx shared that out of 2.2 million kits ordered over a given period of time, they saw a high rate of return, with 1.8 million kits returned.
This cross section of research, advocacy and innovation in STIs and HIV should be a call to action for all of us who see how equity and sexual health cannot be siloed.
P.S. In case you missed it, AVAC recently launched the latest HIV Prevention and Cure Resource Tracking Reports. Find all the details here.
Who’s Driving This Ship?
Over the last year, governments and health leaders have been working to restructure the global health system to ensure pandemic prevention, preparedness, and response. The COVID-19 pandemic forced a reckoning, exposing a deeply inequitable global health system, and advocates, civil society, health workers and leaders representing southern populations, have called on governments to rewrite the world’s contract – in particular, asking Global North governments to finally give up some power and, in the service of preventing and preparing for pandemic threats, agree to join a system that is equitable and aims to prevent health threats everywhere and prepare everyone.
At AVAC, we have put a lot of hope in the processes of the Pandemic Accord, the UN High-Level Meeting (HLM) on Prevention, Preparedness, and Response (PPPR), and the development of a medical countermeasures (MCM) platform. (To understand how these three efforts fit together, see AVAC’s Advocate’s Guide to PPPR.) However, sadly, and in honesty, predictably, many high-income countries seem unwilling to alter the status quo. We see four main sticking points that come down to whether these countries will relinquish control:
Data sharing
Global agreements to share pathogen data and genomic sequencing in the event of a novel pandemic threat represent one of the most important areas of negotiation in these processes. Understandably, many countries are keen to ensure they can have access to data on newly discovered pathogens so they can create a vaccine or treatment as soon as possible and protect their citizens. But since research, manufacturing capacity, and resources are concentrated in the Global North, such an agreement presents a bad deal for countries in the Global South. Such an agreement would require them to share the data they have access to, but continue to be last in line for the vaccines or other interventions that get developed from that data. To add insult to injury, they may well be punished for sharing it, as was the case when the Republic of South Africa shared data on the Omicron mutation of COVID-19 and then saw Global North countries subsequently block entry to their citizens.
But so far, the countries pushing to secure agreements on data sharing refuse to grapple with these concerns. They have not budged and remain unwilling to support language that would ensure access to the beneficial medical countermeasures and that are developed from shared data. While the potential for open science and a platform for data sharing holds promise, these efforts will predictably result in simply exacerbating inequalities unless these agreements beef up commitments around equity. Negotiations on this issue have been tense, with no resolution in sight.
We are quite concerned with the current process of developing an MCM platform that has been proposed by the G7 and G20, along with WHO’s support. The stated aim of the platform is to coordinate equitable development, distribution, and delivery of medical countermeasures for pandemics, including vaccines, therapeutics, diagnostics, and other tools, and to implement the platform in ‘peacetime’ before the next pandemic hits so we’re ready. So far, however, the development process has been largely driven by G7 and G20 countries, both because it will take investment from these countries and because less-resourced countries simply do not have capacity to engage in another PPPR-related process in addition to the Pandemic Accord and UN HLM. Discussions between civil society and country representatives are not happening – while WHO and different agencies have held official meetings with countries, civil society have been relegated to separate discussions. Some global health leaders, from both countries and agencies, have expressed a desire to leave ‘thorny’ issues out of it. But public health advocates and civil society insist that these issues such as intellectual property, clinical trials and R&D prioritization, allocation, the inclusion of marginalized groups, and governance must be considered now before the platform is stood up. It’s unclear who is making the decisions here, but it is certainly not those most burdened by disease.
Financing
The Pandemic Accord draft and the draft UN Declaration on PPPR include few concrete references to PPPR financing targets or finance reform. One of those few is the mention of new-to-the-field Pandemic Fund as a primary resourcing vehicle. This apparent reliance on the Pandemic Fund raises serious questions, as the Fund has offered just $300M in the first round of funding. PPPR agreements that defer finance commitments to the Fund are misguided at best and reveal a lack of ambition to effectively confront pandemic threats. The world currently needs to turn this ship around. Pandemic preparedness must not be an afterthought, a half-hearted boondoggle that only serves the interest of rich countries. All of the issues raised here, in addition to the need to upgrade and expand surveillance systems, increase and strengthen the health workforce, and build up regional manufacturing capacity, need resources to be implemented. On top of those pressing needs, many of the countries that are in most need of investment in pandemic preparedness are straining to manage enormous debt burdens imposed by wealthy countries. Advocates are asking that governments include, in the UN Declaration on PPPR and Pandemic Accord, reference to existing mechanisms such as the Global Fund to Fight AIDS, Tuberculosis, and Malaria (currently the largest funder of PPPR worldwide), the WHO Contingency Fund for Emergencies, and the IMF Resilience and Sustainability Trust as existing vehicles for pandemic preparedness resourcing. PPPR will advance equitably and effectively, and less resources will be needed, if countries commit to leveraging what has already been built in the ongoing responses to HIV, tuberculosis, and malaria. PPPR must learn from twenty years of demonstrated success fighting pandemic and epidemic threats.
So who is driving this ship?
It appears that those who have historically held control have not learned their lesson after yet another global pandemic that abandoned poorer countries and left all of us more vulnerable to the next pandemic. Instead of facing the reality that disease knows no borders and resetting the global health system, those who hold the purse strings seem content to continue with the status quo – hoarding the fruits of science, reinforcing exclusive and hegemonic systems, consolidating power among the few, and keeping health systems fragmented and underfunded. It’s an upside-down system – with those most secure and least in touch with the impact of their decisions in charge. The PPPR ship must be driven by those most burdened by pandemic threats and ongoing epidemics, or we will most certainly face another devastating pandemic and decision-makers will wish they turned it around now.
The Latest Resources From AVAC
AVAC has new resources and information covering mpox, UN negotiations on a declaration on pandemic preparedness, and highlights from the annual South African AIDS Conference (SAAIDS). In addition, be sure to scroll down for upcoming webinars on HIV and STI conferences and more!
Advocacy in Action: An update on the moving pieces of PPPR Pandemic prevention, preparedness and response (PPPR) involves numerous initiatives to ensure the world is ready to respond to existing and future pandemics. UN members are in the midst of negotiating the language of a declaration on PPPR, which will commit heads of state and their governments to agreements on global coordination. And similar negotiations are underway on a global Pandemic Accord.
SA AIDS The 11th annual South Africa AIDS Conference took place in June 20-23 in Durban, South Africa. AVAC and CASPR partners hosted a buzzing Research Literacy Networking Zone with a rich schedule of programs—see the full schedule here, and recordings here. We’re also super excited to report the launch of the Young Women’s HIV Prevention Council at SAAIDS—stay tuned for more about this dynamic group of women soon!
Updated PrEP Product Introduction Country Planning Matrix Check out our updated Product Introduction Country Planning Matrix that tracks the regulatory status of cabotegravir for PrEP and the dapivirine vaginal ring, along with related implementation research, procurement plans, and oral PrEP provision.
ICYMI: Recordings of recent webinars
Mpox: Research, prevention and overcoming disparities—PrEP In Black America, PrEP4All, Treatment Action Group and AVAC co-hosted a webinar with an expert panel who explored the latest research, precautions individuals can take to protect themselves, effectiveness of vaccines, and the ongoing fight to address disparities in infection rates and uptake of vaccines, treatments and tests that impact Black communities. It is important for advocates to remain engaged, and for affected communities to be supported in completing their two-dose mpox vaccine regimens. Listen to the webinar and check out the resources.
PrEP That Booty: The latest on rectal microbicide research for the back door—The latest webinar from The Choice Agenda explored new research on rectal microbicides and advocacy for non-systemic options. Find slides and related resources here and watch for the recording coming soon.
Upcoming Webinars! July 18: ClusterF*#k: Molecular HIV Surveillance, Criminalization, and The Real Risks to PLHIV Register here August 3: Tales from Two Cities: HIV and STI research highlights from IAS in Brisbane and ISSTDR in Chicago Register here
A Recap of Resources: UNAIDS meeting, HVAD webinars and more
In this round up of updates and resources, you’ll find a read-out of the May UNAIDS high-level meeting in Geneva, two webinars that spotlight critical issues for vaccines R&D and the potential of broadly neutralizing antibodies, and an upcoming webinar looking at alternatives to long-acting PrEP. Read on and join us!
The HIV Response at UNAIDS High-level Meeting A high-level meeting in Geneva, held by UNAIDS last month on the margins of the World Health Assembly, brought together advocates and experts through the Global HIV Prevention Coalition to discuss where action is needed most to bolster HIV response and advance global health equity. Read AVAC’s summary of the meeting in our latest P-Values blog.
Vaccines in 2023 and Beyond AVAC hosted two webinars in commemoration of HIV Vaccine Awareness Day. They offer a snapshot on the state of the field for an HIV vaccine, and explore considerations for the development and delivery of vaccines against future pandemics. Check them out below and read more in our HVAD one-pager!
What’s All the Buzz About: mRNA, manufacturing, vaccines access Local production has emerged as an essential part of the solution for ensuring sustainable and equitable supplies of vaccines in low- and middle-income countries. This webinar explored how local manufacturing and the new mRNA Hub in South Africa could facilitate access and support R&D. Check out the summary and recording.
Upcoming PrEP In Black America Presents Mpox Webinar PrEP in Black America alongside a panel of experts will discuss the impact of mpox on Black communities, advocacy and mobilization to keep our communities safe, and information on vaccine effectiveness. Tuesday, June 20 at 2:00 PM to 3:30 PM ET. Register here.
PrEP That Booty: The latest on rectal microbicide research for the back door Most of the coverage of the HIV prevention pipeline is about long-acting, longer-acting, and even longer-acting products that deliver drug throughout the body and require a trained clinician to deliver. However, these attributes are not desirable to many folks, and communities want a range of choices. Learn more about the alternatives at this webinar. Thursday, June 29 at 9:00 AM to 10:30 AM ET. Register here.