The AIDS 2026 conference in Rio de Janeiro, Brazil, starting in less than two weeks, comes at a defining moment for the global HIV response. Under the theme, Rethink. Rebuild. Rise., the conference convenes as the field grapples with funding disruptions, shifting geopolitics and the challenge of sustaining progress while translating scientific breakthroughs into equitable, community-led access. Alongside the latest research, discussions are expected to focus on scaling-up long-acting HIV prevention, strengthening health systems, advancing country ownership, sustaining the research enterprise, and ensuring the HIV response remains grounded in innovation, implementation and investment.
AVAC’s resources below aim to help those attending and those following from afar to navigate the discussion and debate in and around Rio.
Read on for resources and ways to navigate AIDS 2026.
AVAC’s Guides to AIDS 2026

HIV Prevention Session Roadmap
Explore AVAC’s curated roadmap of HIV prevention sessions and key presentations to watch throughout AIDS 2026.

AI and HIV Session Roadmap
AVAC and Audere’s AI & HIV Session Roadmap, features key conference sessions on artificial intelligence in HIV prevention, care, research and global health.
HIV Research & Advocacy Networking Zone

Resources
Resource Hubs

Resource Hub: Lenacapavir for Long-Acting PrEP
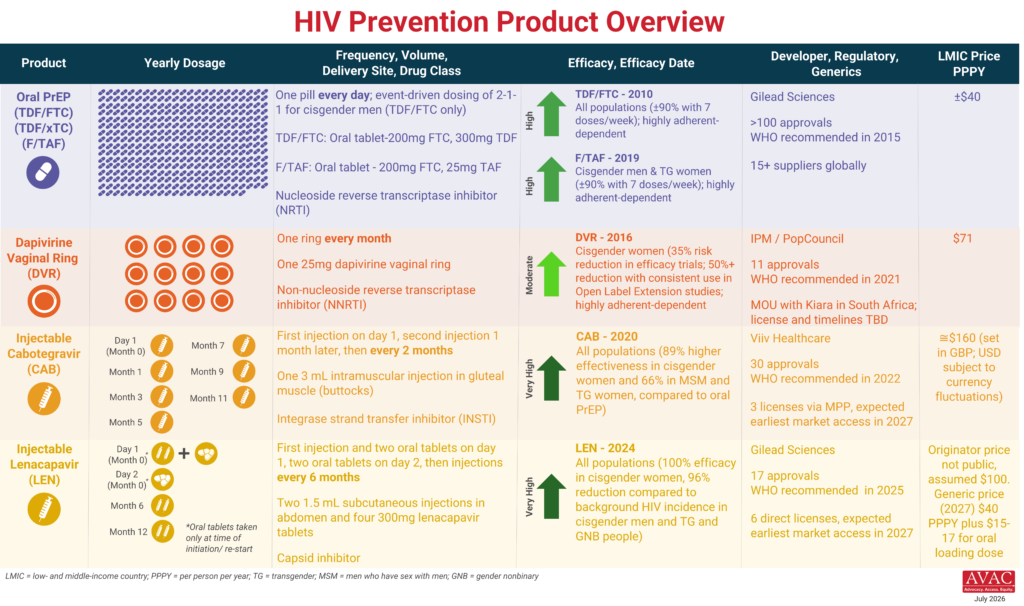
The introduction of injectable lenacapavir for HIV PrEP (LEN) is underway–in some places. While the field is moving faster than it did during the first decade of oral PrEP or the rollout of injectable cabotegravir, ensuring LEN—and future prevention options—reach everyone who needs them will require even greater speed, scale and equity. This resource hub contains all the tools, resources and insights on the latest with LEN rollout.

Resource Hub: MK-8527
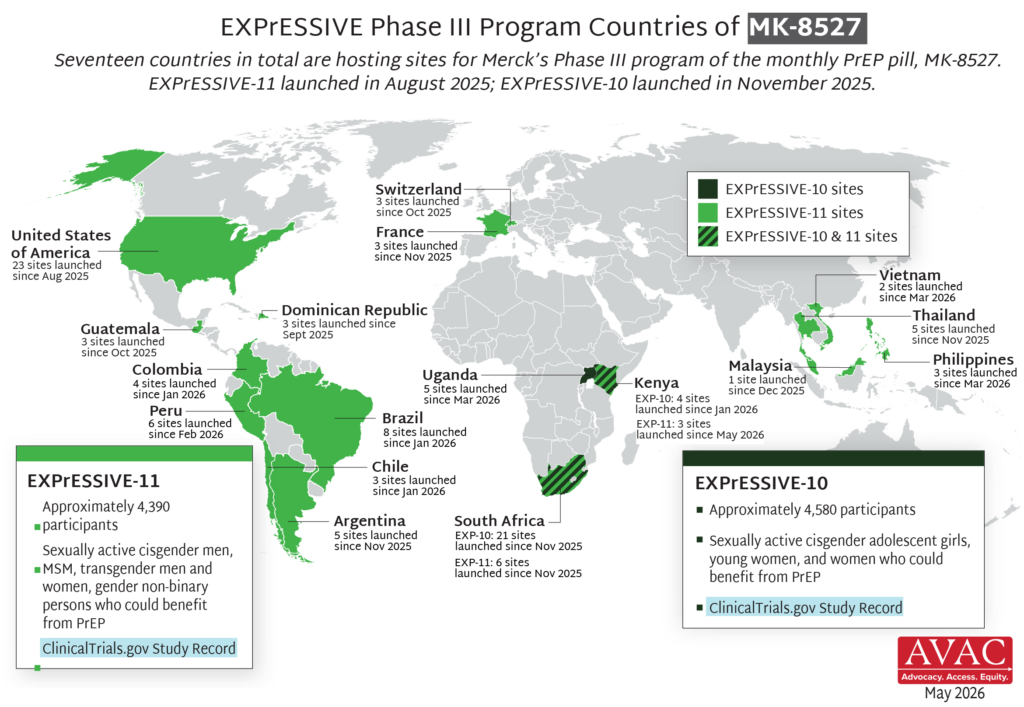
Expanding prevention choice means investing in a diverse pipeline of HIV prevention options. MK-8527 is an investigational antiretroviral (ARV) once-monthly oral PrEP pill currently in Phase III clinical trials. If proven safe and effective, it could offer another important PrEP option. This resource hub provides advocates with an overview of the MK-8527, the science behind it and the latest on its clinical development. It also houses our guide to MK-8527 at AIDS 20206.

Resource Hub: People’s Research Agenda
The People’s Research Agenda (PRA) sets out a people-centered framework for equitable and accelerated R&D and product introduction. This resource hub offers an online, interactive dashboard for tracking, translating, and advocating for HIV prevention research and development (R&D). It also shows where investments align—or fail to align—with community-defined priorities, and spotlights critical gaps in the pipeline of prevention options needed to meet the diverse realities of all populations.
Pre-conferences, Satellites, Sessions and Workshops Featuring AVAC and Partners
- Pre-conference: Advancing HIV prevention science and access
08:00 – 19:00
Hosted by the International AIDS Society, this pre-conference features six sessions showcasing the latest advances in HIV prevention science and access—including the Global Forecast of Long-Acting PrEP Need for Key Populations (2025–2030), developed jointly by GBGMC and AVAC. AVAC board, staff and partners will also explore the science behind next-generation HIV vaccine candidates and how to translate.
Monday, 27 July
- Satellite: Shared pipeline; shared goal: Innovations in long-acting antiretrovirals for PrEP, PEP and treatment
11:30 – 12:30
Organized by AVAC, this session will bring together researchers, product developers, donors, advocates and other partners to explore the future of long-acting antiretroviral (ARV) innovation for PrEP, PEP and treatment.
Tuesday, 28 July
- Symposium: bNAbs for cure: Hope or hype?
10:30-11:30
AVAC Board Member Marina Caskey will present in this symposium exploring the promise—and limitations—of broadly neutralizing antibodies (bNAbs) for HIV cure.
Wednesday, 29 July
- Symposium: Leadership at the tipping point: Protecting the gains and advancing progress in a new era of the HIV response
10:30-11:30
Moderated by AVAC’s Mitchell Warren and HER Voice Fund Ambassador Nomonde Ngema, this symposium explores the future of the global HIV response amid shifting political priorities and an evolving global health landscape.
- Satellite: Choosing impact: Making long-acting HIV prevention a reality for key populations in sub-Saharan Africa
12:00 – 13:00
Organized by Global Black Gay Men Connect (GBGMC) with AVAC and a number of partners participating, this session will examine strategies to sustain and expand HIV prevention for key populations as long-acting prevention options become available.
- Satellite: To fund or not to fund: Pathways and proof points to sustaining HIV prevention as part of integrated approaches and health financing reforms
18:00 – 19:30
Organized by PATH, AVAC, UNAIDS, WHO, Unitaid, APCOM, ICWEA, Harvard, Frontline AIDS and the Elton John AIDS Foundation, this session will examine the growing HIV prevention funding crisis and what’s needed to sustain progress.
Thursday, 30 July
- Workshop: Skills Lab: Community-led monitoring
12:00 – 13:30
Facilitated by the International Treatment Preparedness Coalition (ITPC), NACOSA, the Network of Journalists Living with HIV (JONEHA) and community monitoring experts, including AVAC Senior Advisor Maureen Luba, this interactive workshop will strengthen practical skills in community-led monitoring (CLM).
- Symposium: From community to innovation to scale
16:30 – 17:30
AVAC’s Grace Kumwenda will join community leaders, researchers, clinicians, policymakers and funders to discuss the partnerships, inclusive research and implementation strategies needed to accelerate innovation and ensure equitable access from the outset.
- Satellite: From choice to impact: Long-acting and multipurpose HIV prevention technologies
18:00 – 19:30
Hosted by IPM South Africa, AVAC and Access Bridge’s Kate Segal and Ascend Futures Foundation’s Chilufya Kasanda will join researchers, advocates, implementers and policymakers to examine the latest scientific advances, implementation strategies and pathways to equitable access for long-acting options and MPTs.
Friday, July 31
- Symposium: The promises of long-acting injectable PrEP for HIV prevention
10:30 – 11:30
Access Bridge Executive Director Wawira Nyagah share community perspectives on early implementation of injectable cabotegravir and lenacapavir, identifying remaining gaps, and discussing strategies to accelerate equitable rollout.
Follow Us
AVAC will be covering conversations and events at the conference. Be sure to follow along on social and find updates on our AIDS 2026 page.
- BlueSky: @avac.org
- Instagram: @hivpxresearch
- LinkedIn: AVAC (AIDS Vaccine Advocacy Coalition)