Since 2012, AVAC has worked to strengthen the capacity of journalists to report on HIV prevention research and global health and science topics. Through its flagship Media Science Café Program, AVAC partners with health media associations in Kenya, Malawi, Tanzania, Uganda, Zambia and Zimbabwe to connect journalists with subject matter experts—researchers, policymakers and advocates—and help build the relationships needed to foster accurate and informed reporting of HIV, COVID and emerging health and science issues.
Media Science Cafes
AVAC Capability Statement
Joint Statement on the April 18th Revised Pandemic Accord Draft
The Coalition of Advocates for Global Health and Pandemic Preparedness, a group of organizations advocating for a holistic and equitable approach in pandemic preparedness, offers several revisions to the April 18 revised Pandemic Accord draft.
Announcing the 2024/25 AVAC Advocacy Fellows
We are pleased to announce our 13th class of the flagship AVAC Advocacy Fellows Program for 2024-2025! This group of seven advocates will participate in an 18-month program that supports their advocacy efforts, invests in the further development of their skills, shapes the agenda for HIV prevention research, and influences how quickly new interventions move into policy and programs in their communities and countries.
Samuel Anyula Gorigo
Samuel Anyula Gorigo, also known as Sam, is a dedicated healthcare professional with over five years of experience specializing in HIV prevention, care and treatment, as well as sexually transmitted infections. With a strong background in public health for key populations and advocacy for health rights championing accessibility, equity and inclusivity. Leading the clinical arm at HOYMAS Kenya, my project seeks to strengthen HIV prevention while amplifying anal health and HPV vaccine accessibility for gay, bisexual and other men who have sex with men (GBMSM). My advocacy pushes for reforms in health policies and guidelines to be inclusive and equitable. Through the AVAC 2024 Advocacy Fellowship, I intend to address health service gaps for GBMSM, advocating for comprehensive and responsive health policies that cater to the unique needs of key populations, ensuring equitable health systems for all.
Media/Advocacy
- I lead Kenya’s first anal health screening programme, the crisis is worse than you think, The Star
- HPV in Kenya Factsheet
- Why Men and Boys Must be Involved in Slaying HIV, SAYANSI
- HIV and HPV Take Devastating Tool on Homosexuals in Kenya — The Standard
- HPV: The need to confront men’s anal health — The Star
- Speaking the Unspeakable: The need to confront men’s sexual health — The Nation
- Toward Improving Anal Health Care Among GBMSM in Kenya: Lessons from a patient’s illness, treatment and recovery journey — Global Public Health
Ezra Meme
Ezra is a public health advocate with a background in combating HIV-related stigma and contributing to the innovation of the HIV Stigma Index. His experience in Monitoring and Evaluation of HIV/TB care and treatment projects drives his evidence-based approach and supports his effort to integrate HIV prevention efforts with pandemic preparedness activities. As an AVAC 2024 Advocacy Fellow, Ezra aims to bolster Uganda’s response to emerging pandemic threats. As the country develops the New Action Plan for Health and Security, a unique opportunity is presented for budget advocacy and monitoring compliance with International Health Regulations. Through collaborative efforts, and fostering community engagement, Ezra hopes his project can empower vulnerable populations and build resilience against future health crises in our push for global health equity.
Media/Advocacy
April Webinars!
This month we will host six webinars on a wide range of important issues, including choice in HIV prevention, PrEP in cisgender women, criminalization and HIV, syphilis in the US and DoxyPEP. Scroll down for what’s coming up later this week and later this month.
The More We Know: Evolving our understanding of PrEP for cisgender women
April 5, 9:00 – 10:30 am EST
Science and real-world experience continue to demand a re-assessment of our collective understanding of the safety and effectiveness of PrEP options for women, including oral, vaginal ring, and injectable options. Join us, Jeanne Marrazzo of NIAID, Joyce Ng’ang’a of WACI Health and Raniyah Copeland of Equity & Impact Solutions for a conversation with The Choice Agenda.
Watching the Watcher: Intersections of surveillance and criminalization in HIV and reproductive health care
April 9, 10:00 – 11:30 am EST
Positive Women’s Network-USA and The Choice Agenda invite you to join us for a webinar featuring leaders in digital technology, HIV advocacy, and abortion criminalization to examine the existential threat of our ongoing blurred boundaries between public health and policing.
STI Awareness Week is April 14 – 20!
Join us for two webinars focused on syphilis and DoxyPEP. These webinars are intended for health care providers, civil society organizations, public health officials, and others working in the STI/HIV fields.
Discussing Early Results from the SEARCH Dynamic Choice Study
April 23, 10:00 – 11:30 am EST
Join AVAC and Professor Moses Kamya of Makerere University to find out why the early results of the SEARCH Dynamic Choice study were some of the most exciting to come out of CROI in 2024.
Conducted in Kenya and Uganda, the study offered oral PrEP, PEP or injectable cabotegravir to both men and women, and an option to switch products.
We Can’t End HIV in the United States Without Equitable PrEP Access: strategies for success
April 26, 1:00 – 2:30 pm EST
Join HIVMA, PrEP4All and The Choice Agenda, as we assess some of the key challenges to delivering PrEP in the United States equitably, including cost, the complexities of our health care system, and other factors that inhibit uptake amongst the most vulnerable communities. Strategies to address these challenges will be offered, with lots of time for QA, discussion and much-needed debate. Please join us!
Our Partnership Network
Capability Statement
AVAC’s greatest strengths lie in its ability to convene diverse stakeholders in the fight against HIV and its dedication to bolstering civil society coalitions for effective advocacy.
STIWatch Newsletter, March 2024
The first quarter of 2024 ends with new research and questions on the future directions of STI vaccines and diagnostics. The Conference on Retroviruses and Opportunistic Infections (CROI) was the setting for positive news on the potential for early use of doxycycline to prevent STIs (DoxyPEP) in real-world settings and questions about its effectiveness in cisgender women given major evidence gaps. Important discussions and debates continued around the issue of antimicrobial resistance (AMR), as the field continues to grapple with the rollout of DoxyPEP. Presentations at CROI also highlighted the need for new diagnostics for syphilis as infections continue to increase globally and the need for STI advocacy efforts to ensure these infections get the attention and funding needed to develop vaccines and diagnostics that can prevent, detect, and treat these infections!
In January, the US Centers for Disease Control and Prevention (CDC) released the STI surveillance data from 2022, which showed an increase in chlamydia and syphilis cases from 2021. Gonorrhea cases decreased between 2021 and 2022 by 9%. Alarmingly, 2022 congenital syphilis cases increased by 30% from 2021, signaling an urgent need for novel prevention, treatment, and testing methods.
In Australia, a group of researchers published a response to the Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine’s October 2023 statement on the use of DoxyPEP in Australia. The authors point to the potential threat of increasing AMR and the urgent need to implement measures to monitor DoxyPEP use and its impact.
Read on for upcoming webinars, must-read resources supporting advocacy for improved funding and commitments for STI vaccines and diagnostics. Afterwards, test your knowledge with AVAC’s new STI Trivia quiz.
New Report! STIs: A Review of the 2022 Vaccine and Diagnostic R&D Pipeline and Investments
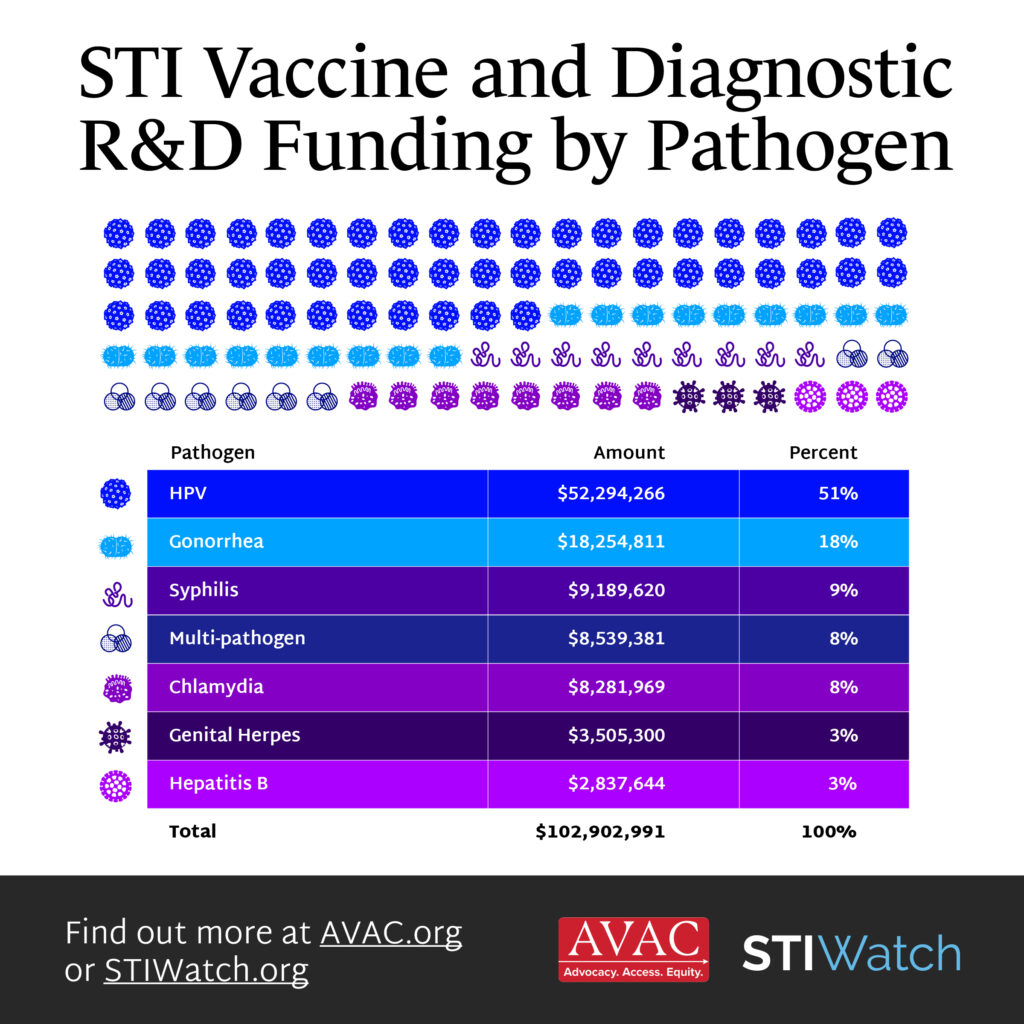
A new AVAC report tracks funding trends in vaccine and diagnostics R&D, and pipeline investments for some of the most common STIs, including chlamydia, genital herpes, gonorrhea, hepatitis B, human papillomavirus (HPV), syphilis, and trichomoniasis. The report finds that STI research remains underfunded and neglected compared to other infectious diseases. Read the report to learn more.
STI Advocacy Updates

AVAC spoke with two cervical cancer advocates, Tamika Felder and Karen Nakawala, in January as part of its cervical cancer webinar series. Felder and Nakawala are breaking taboos and saving lives by empowering people to share their stories of survivorship and senseless loss.
Felder, founder of Cervivor, Inc., was diagnosed with cervical cancer at 25, and turned her struggle into a mission, providing resources and a platform for those affected by the disease. Her impactful work and advocacy inspired Nakawala to found the Teal Sisters Foundation in 2020, following her successful treatment for cervical cancer. To learn more about Tamika and Karen, watch AVACs cervical cancer webinar. Thank you, Tamika and Karen for all that you do!
January 18 marked HPV Awareness Day. AVAC and TogetHER for Health released an updated call to action to improve HPV vaccination among people living with HIV. In total, 31 organizations signed on to this call, urging global leadership to increase access to lifesaving HPV vaccines for people living with HIV.
Upcoming Events
STI Awareness Week is April 14 – 20!
Join us for two webinars focused on syphilis and DoxyPEP. These webinars are intended for health care providers, civil society organizations, public health officials, and others working in the STI/HIV fields.
September 2024 STI Conferences
REGISTRATION IS NOW OPEN FOR TWO IMPORTANT STI CONFERENCES IN SEPTEMBER – WHICH UNFORTUNATELY ARE RUNNING CONCURRENTLY IN DIFFERENT PARTS OF THE WORLD!
The 2024 STI Prevention Conference will bring 1,200 conference attendees to Atlanta, Georgia, from September 16-19, 2024. Abstracts are being accepted until March 29.
The 25th IUSTI World Congress will take place September 17-20, 2024, in Sydney, Australia, and provide an opportunity to meet, discuss and learn about the latest research and innovation in sexual and reproductive health.
What We’re Reading and Resources
- Testing, testing: the advancing diagnostics for sexually transmitted infections. Diagnostics are urgently needed to detect STIs and this article examines several that are on the horizon. A US-Based company, Qvin is developing the Q-pad, a diagnostic menstrual pad with a removable strip to identify signs of diabetes and symptoms of high-risk human papillomavirus. Daye, a UK based gynecological start-up, launched a diagnostic product that is a tampon with the ability to screen for STIs. These advancements are exciting and serve as a reminder that advocacy is needed to ensure these products get to the people who need them.
- CARB-X Funds Visyby Medical to Develop a portable rapid diagnostic for Gonorrhea Including Antibiotic Susceptibility Combating Antibiotic-Resistant Bacteria Biopharmaceutical Accelerator (CARB-X) will award up to US$1.8 million to biotechnology company, Visby Medical, to develop a portable rapid polymerase chain reaction (PCR) diagnostic to detect gonorrhea and its susceptibility to ciprofloxacin, a former frontline oral antibiotic that can no longer treat gonorrhea infections resistant to this medication. Funding will also support development of a test for gonorrhea, chlamydia, and trichomoniasis in men based on urine samples.
- Syphilis Complicating Pregnancy and Congenital Syphilis. This manuscript provides a review of syphilis during pregnancy and congenital syphilis. As syphilis and congenital syphilis infections continue to rise, novel approaches are needed to detect, prevent, and treat infections. Because syphilis disproportionately affects populations with limited access to healthcare, new and improved diagnostics and therapeutics will need to be embedded within a health framework that prioritizes equity to improve the diagnosis and treatment of congenital syphilis, a preventable disease.
- Near-to-patient-testing to inform targeted antibiotic use for sexually transmitted infections in a public sexual health clinic: the NEPTUNE cohort study. This study examines the effectiveness of a novel lateral flow assay for point-of-care detection of gonorrhea among people with symptoms. Lateral flow assays are tests that can detect the presence of proteins or antigens for specific infections, like COVID-19 and HIV. This test had excellent clinical sensitivity and specificity in detecting gonorrhea among male and female patients with symptoms. A test like this could provide an important tool to better detect infections in settings without direct access to laboratory testing and reduce overtreatment.
- Breaking Barriers in STI Clinical Management: Addressing Resistance Challenges and Incorporating New Diagnostic Approaches. This on-demand webinar features Dr. Van Der Pol and Dr. William Geisler who share their insights on crucial aspects of STI clinical management, focusing on resistance challenges and new diagnostic approaches.
To learn more about AVAC’s STI Program, visit STIWatch.org and avac.org/sti. Email [email protected] for questions or additional information. And to sign up for specific updates on STIs, click here.
STIWatch Newsletter, March 2024
The first quarter of 2024 ends with new research and questions on the future directions of STI vaccines and diagnostics. The Conference on Retroviruses and Opportunistic Infections (CROI) was the setting for positive news on the potential for early use of doxycycline to prevent STIs (DoxyPEP) in real-world settings and questions about its effectiveness in cisgender women given major evidence gaps. Important discussions and debates continued around the issue of antimicrobial resistance (AMR), as the field continues to grapple with the rollout of DoxyPEP. Presentations at CROI also highlighted the need for new diagnostics for syphilis as infections continue to increase globally and the need for STI advocacy efforts to ensure these infections get the attention and funding needed to develop vaccines and diagnostics that can prevent, detect, and treat these infections!
In January, the US Centers for Disease Control and Prevention (CDC) released the STI surveillance data from 2022, which showed an increase in chlamydia and syphilis cases from 2021. Gonorrhea cases decreased between 2021 and 2022 by 9%. Alarmingly, 2022 congenital syphilis cases increased by 30% from 2021, signaling an urgent need for novel prevention, treatment, and testing methods.
In Australia, a group of researchers published a response to the Australasian Society for HIV, Viral Hepatitis and Sexual Health Medicine’s October 2023 statement on the use of DoxyPEP in Australia. The authors point to the potential threat of increasing AMR and the urgent need to implement measures to monitor DoxyPEP use and its impact.
Read on for upcoming webinars, must-read resources supporting advocacy for improved funding and commitments for STI vaccines and diagnostics. Afterwards, test your knowledge with AVAC’s new STI Trivia quiz.
New Report! STIs: A Review of the 2022 Vaccine and Diagnostic R&D Pipeline and Investments
A new AVAC report tracks funding trends in vaccine and diagnostics R&D, and pipeline investments for some of the most common STIs, including chlamydia, genital herpes, gonorrhea, hepatitis B, human papillomavirus (HPV), syphilis, and trichomoniasis. The report finds that STI research remains underfunded and neglected compared to other infectious diseases. Read the report to learn more.
STI Advocacy Updates
AVAC spoke with two cervical cancer advocates, Tamika Felder and Karen Nakawala, in January as part of its cervical cancer webinar series. Felder and Nakawala are breaking taboos and saving lives by empowering people to share their stories of survivorship and senseless loss.
Felder, founder of Cervivor, Inc., was diagnosed with cervical cancer at 25, and turned her struggle into a mission, providing resources and a platform for those affected by the disease. Her impactful work and advocacy inspired Nakawala to found the Teal Sisters Foundation in 2020, following her successful treatment for cervical cancer. To learn more about Tamika and Karen, watch AVACs cervical cancer webinar. Thank you, Tamika and Karen for all that you do!
January 18 marked HPV Awareness Day. AVAC and TogetHER for Health released an updated call to action to improve HPV vaccination among people living with HIV. In total, 31 organizations signed on to this call, urging global leadership to increase access to lifesaving HPV vaccines for people living with HIV.
Upcoming Events
STI Awareness Week is April 14 – 20!
Join us for two webinars focused on syphilis and DoxyPEP. These webinars are intended for health care providers, civil society organizations, public health officials, and others working in the STI/HIV fields.
September 2024 STI Conferences
Registration is now open for two important STI conferences in September – which unfortunately are running concurrently in different parts of the world!
The 2024 STI Prevention Conference will bring 1,200 conference attendees to Atlanta, Georgia, from September 16-19, 2024. Abstracts are being accepted until March 29.
The 25th IUSTI World Congress will take place September 17-20, 2024, in Sydney, Australia, and provide an opportunity to meet, discuss and learn about the latest research and innovation in sexual and reproductive health.
What We’re Reading and Resources
- Testing, testing: the advancing diagnostics for sexually transmitted infections. Diagnostics are urgently needed to detect STIs and this article examines several that are on the horizon. A US-Based company, Qvin is developing the Q-pad, a diagnostic menstrual pad with a removable strip to identify signs of diabetes and symptoms of high-risk human papillomavirus. Daye, a UK based gynecological start-up, launched a diagnostic product that is a tampon with the ability to screen for STIs. These advancements are exciting and serve as a reminder that advocacy is needed to ensure these products get to the people who need them.
- CARB-X Funds Visyby Medical to Develop a portable rapid diagnostic for Gonorrhea Including Antibiotic Susceptibility Combating Antibiotic-Resistant Bacteria Biopharmaceutical Accelerator (CARB-X) will award up to US$1.8 million to biotechnology company, Visby Medical, to develop a portable rapid polymerase chain reaction (PCR) diagnostic to detect gonorrhea and its susceptibility to ciprofloxacin, a former frontline oral antibiotic that can no longer treat gonorrhea infections resistant to this medication. Funding will also support development of a test for gonorrhea, chlamydia, and trichomoniasis in men based on urine samples.
- Syphilis Complicating Pregnancy and Congenital Syphilis. This manuscript provides a review of syphilis during pregnancy and congenital syphilis. As syphilis and congenital syphilis infections continue to rise, novel approaches are needed to detect, prevent, and treat infections. Because syphilis disproportionately affects populations with limited access to healthcare, new and improved diagnostics and therapeutics will need to be embedded within a health framework that prioritizes equity to improve the diagnosis and treatment of congenital syphilis, a preventable disease.
- Near-to-patient-testing to inform targeted antibiotic use for sexually transmitted infections in a public sexual health clinic: the NEPTUNE cohort study. This study examines the effectiveness of a novel lateral flow assay for point-of-care detection of gonorrhea among people with symptoms. Lateral flow assays are tests that can detect the presence of proteins or antigens for specific infections, like COVID-19 and HIV. This test had excellent clinical sensitivity and specificity in detecting gonorrhea among male and female patients with symptoms. A test like this could provide an important tool to better detect infections in settings without direct access to laboratory testing and reduce overtreatment.
- Breaking Barriers in STI Clinical Management: Addressing Resistance Challenges and Incorporating New Diagnostic Approaches. This on-demand webinar features Dr. Van Der Pol and Dr. William Geisler who share their insights on crucial aspects of STI clinical management, focusing on resistance challenges and new diagnostic approaches.
To learn more about AVAC’s STI Program, visit STIWatch.org and avac.org/sti. Email [email protected] for questions or additional information. And to sign up for specific updates on STIs, click here.
New Podcast Episode: Decolonizing Global Health
Dear Advocate,
Investing in the long-term success of African leadership is essential to breaking cycles that perpetuate inequity and that stall progress in the HIV response. In our newest episode of PxPulse, we explore why and how the decisions that shape global health must be made by those facing the greatest risks. As the world evaluates the pandemic response and debates on decolonizing global health gain momentum, equity in global health has never been more urgent.
For more than seven years, COMPASS Africa, a civil society coalition of 29 organizations working in three countries as well as regionally and globally, has used data-driven advocacy to improve the HIV response with high-impact campaigns. In January, the coalition underwent a major transition, with Pangaea Zimbabwe assuming the role of secretariat (previously held by AVAC), marking a historic milestone in the development of innovative models for power-sharing in coalition and an important step toward decolonizing global health. These changes in COMPASS come as other efforts, such as negotiations on the Pandemic Accord, are struggling to advance, uphold or safeguard equity.
Now is the time to test new models. In Decolonizing Global Health: Dr. Madhukar Pai and COMPASS Africa Tell Us Why and How, we explore what it takes to invest in equity and power sharing.
New Episode of PxPulse!

This episode of PxPulse features global health leader, Dr. Madhukar Pai, along with two leaders of COMPASS Africa, Francis Luwole and Barbra Ncube, talking about new models of power-sharing.
Listen now!
Tune in to Hear
- Dr. Madhu Pai, a Canada Research Chair of Epidemiology & Global Health at McGill University and Co-Editor-in-Chief of PLOS Global Health
- Francis Luwole is the Tanzania Country Coordinator for COMPASS Africa
- Barbra Ncube is Programs Quality Coordinator for Pangaea Zimbabwe and member of COMPASS Africa
Join the Conversation

To continue the conversation, register for the March 26 Choice Agenda webinar, Decolonizing Global Public Health: Exploring the how, from now, til as long as it takes.